

Comparing the effectiveness of universal admission testing and risk-based testing at emergency admission for preventing nosocomial COVID-19: a multicenter retrospective cohort study in Japan
- PMID: 39434373
- PMCID: PMC11717481
- DOI: 10.1017/ice.2024.161
Comparing the effectiveness of universal admission testing and risk-based testing at emergency admission for preventing nosocomial COVID-19: a multicenter retrospective cohort study in Japan
Abstract
Objective: To compare the effectiveness of universal admission testing (UAT) and risk-based testing (RBT) in preventing nosocomial coronavirus disease 2019 (COVID-19) after the implementation of strict infection control measures.
Design: Retrospective multicenter cohort study.
Setting: Five community hospitals in Japan.
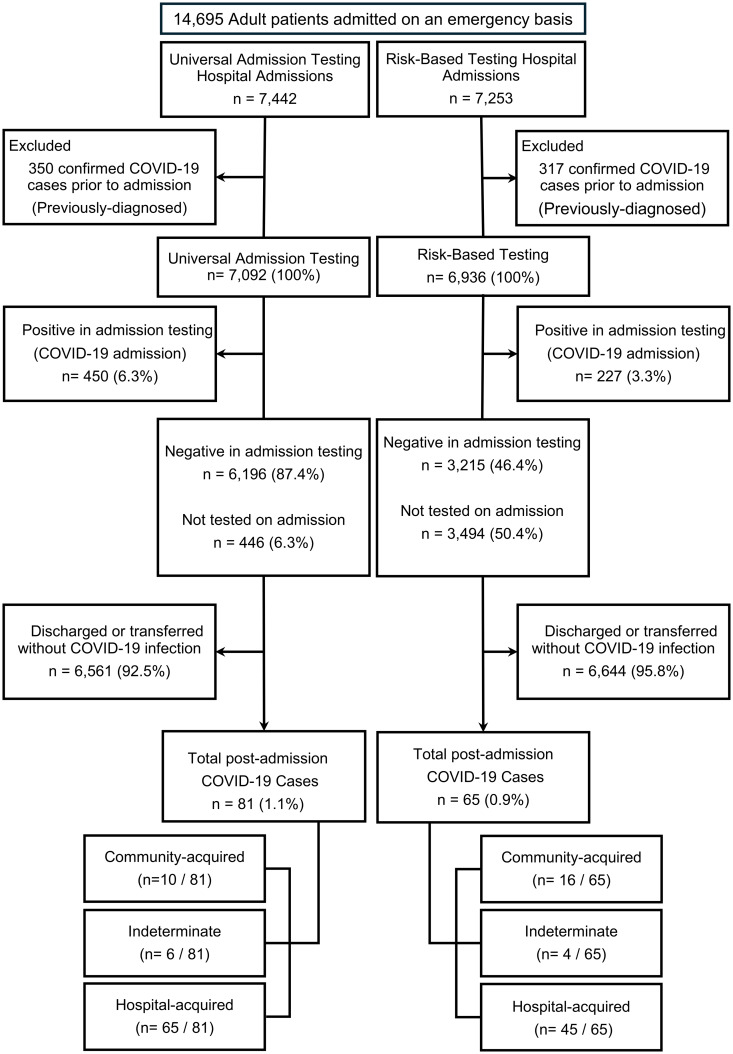
Patients: 14,028 adult patients admitted emergently from June 1, 2022, to January 31, 2023.
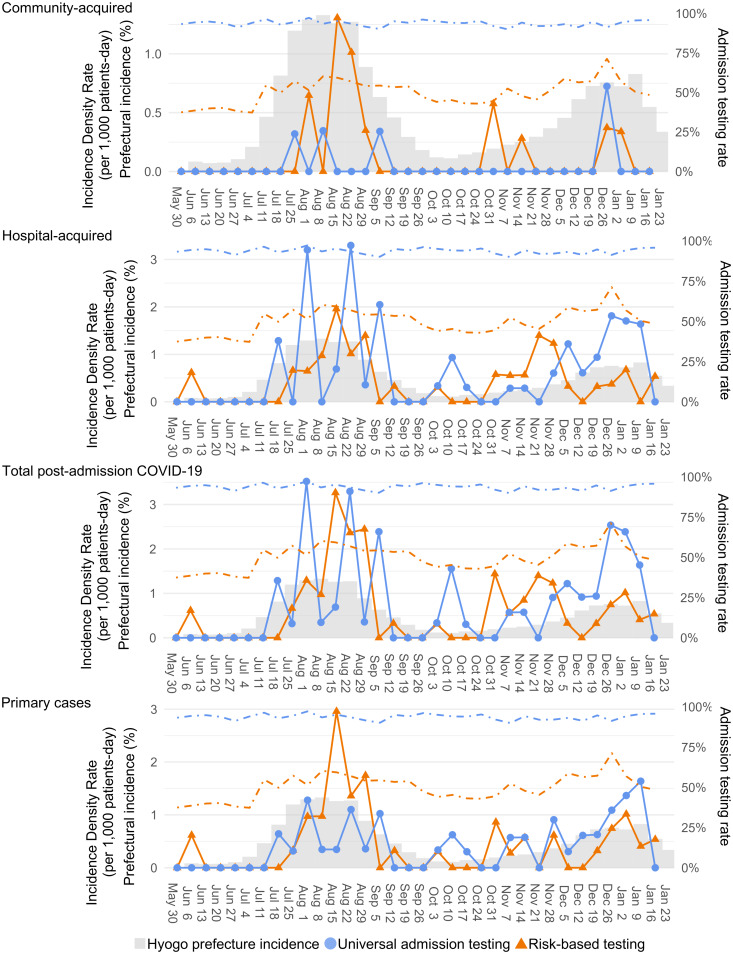
Methods: We calculated crude incidence density rates of community-acquired COVID-19 (positive test ≤4 days postadmission), hospital-acquired COVID-19 (positive test ≥8 days postadmission), total postadmission COVID-19 (all cases of positive test postadmission), and primary cases (sporadic and index cases). A generalized estimating equation model was used to adjust for local incidence (new COVID-19 patients per 100,000 population), single-bed room proportion, and admission proportion of patients older than 65 years.
Results: The weekly local incidence in the study areas was less than 1,800 per 100,000 population (1.8%). Two hospitals implemented RBT and 3 implemented UAT. The median admission testing rate was higher in the UAT group than in the RBT group (95% vs 55%; difference 45.2%, 95% CI, 40.3%-48.8%). Crude and adjusted analyses revealed no significant associations between incidence density rates (IRR; >1 indicates higher incidence with UAT) and admission strategies for any of the outcomes: community-acquired cases (adjusted IRR = 1.23; 95% CI, 0.46-3.31), hospital-acquired cases (1.46; 0.80-2.66), total postadmission COVID-19 (1.22; 0.79-1.87), and primary cases (0.81; 0.59-1.12).
Conclusions: Compared with risk-based testing, universal admission testing may have limited additional benefits in preventing nosocomial COVID-19 transmission during a period of low-moderate local incidence.
Conflict of interest statement
All authors report no conflicts of interest relevant to this article.
Figures
Similar articles
-
Assessment of Hospital-Onset SARS-CoV-2 Infection Rates and Testing Practices in the US, 2020-2022.JAMA Netw Open. 2023 Aug 1;6(8):e2329441. doi: 10.1001/jamanetworkopen.2023.29441. JAMA Netw Open. 2023. PMID: 37639273 Free PMC article.
-
Coronavirus disease 2019 (COVID-19) universal admission screening in patients and companions in Taiwan from May 2021 to June 2022: A nationwide multicenter study.Infect Control Hosp Epidemiol. 2024 Jan;45(1):68-74. doi: 10.1017/ice.2023.144. Epub 2023 Jul 18. Infect Control Hosp Epidemiol. 2024. PMID: 37462097 Free PMC article.
-
Evaluating the impact of testing strategies for the detection of nosocomial COVID-19 in English hospitals through data-driven modeling.Front Med (Lausanne). 2023 Oct 11;10:1166074. doi: 10.3389/fmed.2023.1166074. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37928455 Free PMC article.
-
Universal screening for SARS-CoV-2 infection: a rapid review.Cochrane Database Syst Rev. 2020 Sep 15;9(9):CD013718. doi: 10.1002/14651858.CD013718. Cochrane Database Syst Rev. 2020. PMID: 33502003 Free PMC article.
-
International travel-related control measures to contain the COVID-19 pandemic: a rapid review.Cochrane Database Syst Rev. 2021 Mar 25;3(3):CD013717. doi: 10.1002/14651858.CD013717.pub2. Cochrane Database Syst Rev. 2021. PMID: 33763851 Free PMC article.
References
-
- Klompas M, Baker MA, Rhee C. Is nosocomial SARS-CoV-2 still worth preventing? JAMA Netw Open 2023;6:e2344704. - PubMed
-
- Williams VR, Chan CK, Chan AK, Kozak R, Leis JA. Impact of universal admission testing for severe acute respiratory coronavirus 2 (SARS-CoV-2) in era of the omicron variant. Infect Control Hosp Epidemiol 2023;44:102–105. - PubMed
LinkOut - more resources
Full Text Sources
