

Efficacy and safety of gene therapy with onasemnogene abeparvovec in children with spinal muscular atrophy in the D-A-CH-region: a population-based observational study
- PMID: 39434961
- PMCID: PMC11492610
- DOI: 10.1016/j.lanepe.2024.101092
Efficacy and safety of gene therapy with onasemnogene abeparvovec in children with spinal muscular atrophy in the D-A-CH-region: a population-based observational study
Abstract
Background: Real-world data on gene addition therapy (GAT) with onasemnogene abeparvovec (OA), including all age groups and with or without symptoms of the disease before treatment are needed to provide families with evidence-based advice and realistic therapeutic goals. Aim of this study is therefore a population-based analysis of all patients with SMA treated with OA across Germany, Austria and Switzerland (D-A-CH).
Methods: This observational study included individuals with Spinal Muscular Atrophy (SMA) treated with OA in 29 specialized neuromuscular centers in the D-A-CH-region. A standardized data set including WHO gross motor milestones, SMA validated motor assessments, need for nutritional and respiratory support, and adverse events was collected using the SMArtCARE registry and the Swiss-Reg-NMD. Outcome data were analyzed using a prespecified statistical analysis plan including potential predictors such as age at GAT, SMN2 copy number, past treatment, and symptom status.
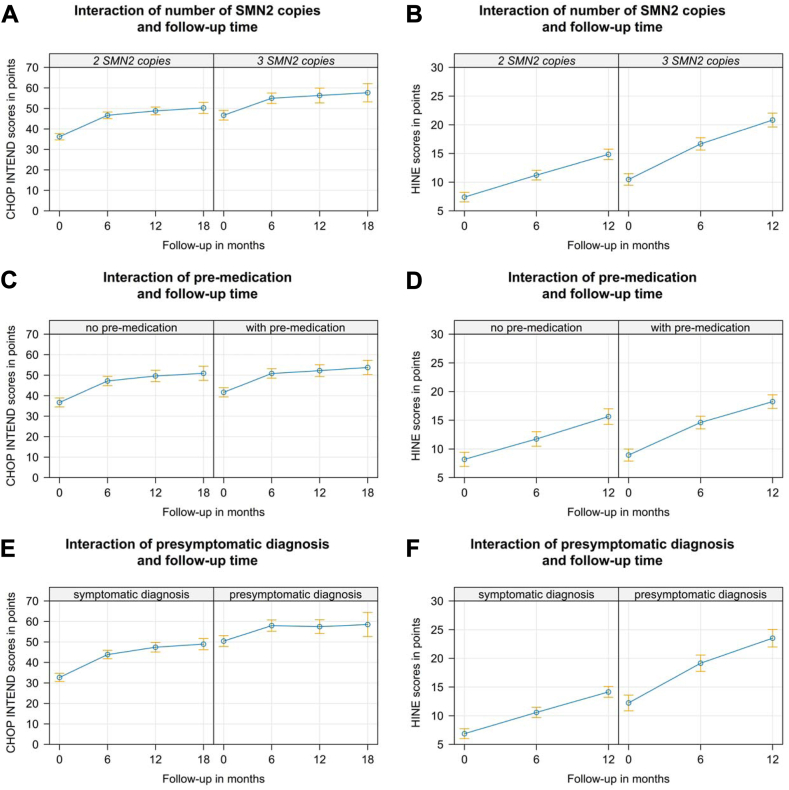
Findings: 343 individuals with SMA (46% male, 54% female) with a mean age at OA of 14.0 months (range 0-90, IQR 20.0 months) were included in the analysis. 79 (23%) patients were clinically presymptomatic at the time of treatment. 172 (50%) patients received SMN2 splice-modifying drugs prior to GAT (risdiplam: n = 16, nusinersen: n = 154, both: n = 2). Functional motor improvement correlated with lower age at GAT, with the best motor outcome in those younger than 6 weeks, carrying 3 SMN2 copies, and being clinically presymptomatic at time of treatment. The likelihood of requiring ventilation or nutritional support showed a significantly increase with older age at the time of GAT and remained stable thereafter. Pre-treatment had no effect on disease trajectories. Liver-related adverse events occurred significantly less frequently up to 8 months of age. All other adverse events showed an even distribution across all age and weight groups.
Interpretation: Overall, motor, respiratory, and nutritional outcome were dependent on timing of GAT and initial symptom status. It was best in presymptomatic children treated within the first six weeks of life, but functional motor scores also increased significantly after treatment in all age groups up to 24 months. Additionally, OA was best tolerated when administered at a young age. Our study therefore highlights the need for SMA newborn screening and immediate treatment to achieve the best possible benefit-risk ratio.
Funding: The SMArtCARE and Swiss-Reg-NMD registries are funded by different sources (see acknowledgements).
Keywords: Gene addition therapy; Gene therapy; Onasemnogene abeparvovec; SMA; Spinal muscular atrophy; Zolgensma.
© 2024 The Author(s).
Conflict of interest statement
No author received financial support for the present manuscript. CW received honoraria for presentations and/or travel support from Novartis, Roche and Biogen and participated on advisory boards for Novartis, Roche and Biogen. JF received honoraria from Novartis for presentations. AB received honoraria for presentations from Roche and Pfizer and attend advisory boards for Roche and Pfizer. SI received honoraria for presentations and advisory board meetings from Novartis and Roche. OS received honoraria from Biogen, support for attending meetings from Novartis and participated on an advisory board for Novartis. GB received honoraria for advisory boards and/or presentations from Novartis, Roche and Biogen and support for attending meetings from Novartis. MvdH received grants from Deutsche Gesellschaft für Muskelkranke and Innovationsfond (INTEGRATE ATMP and KoCoN), honoraria from Pfizer, Biogen and PTC Therapeutics, and participated on advisory boards for Roche, Sarepta, Novartis, and Pfizer. RAH received consulting fees from Biogen and honoraria for presentations from Novartis, and participated on advisory boards by Novartis and Roche. KG participated on an industry symposium and an advisory board by Novartis. JK received funding for clinical research from Biogen, Novartis, Roche, ScholarRock and Biohaven, consulting fees from Biogen, Novartis and Roche, payment for educational activities from Biogen, Novartis and Roche and attended a data safety monitoring board for Biogen. AP received research funding form Roche, Novartis and Biogen. MFB received consulting fees for advisory boards from Roche, Novartis and Biogen and payment for presentations from Novartis and Biogen. GS received honoraria for a case report and participated on an advisory board for Novartis. US received honoraria for presentations from Biogen, Novartis and Roche and support for attending meetings from Roche and Novartis. BP received honoraria for a presentation from Biogen and participated on advisory boards for Novartis and Biogen. RT received honoraria for presentations from Desitin, PTC and Roche and participated on advisory boards for PTC, Roche and Santhera. VH attended an adivisory board for Biogen. MB received compensation for advisory boards and speakers honoraria from Novartis, Biogen and Roche and compensation for travel costs to meetings from Roche. AK is clinical lead of the Swiss Reg NMD, attended advisory board meetings of Novartis and received honorarium for a presentation by Novartis. AE received honoraria and payment for expert testimony from Biogen, Roche and Novartis, support for attending meetings from Biogen and Roche and participated on an advisory board for Biogen, Roche and Novartis. GMS participated on advisory boards from Biogen, Novartis and Roche and is member of the steering board for Swiss-Reg-NMD. SC received payment for a presentation. JJ received compensation for advisory boards and funding for travel or speaker honoraria from Avexis/Novartis, Biogen, IFT, Roche, PTC, Pfizer and Sarepta Therapeutics. AZ received compensation for advisory boards and funding for travel or speaker honoraria from Avexis/Novartis, Biogen, ITF, Roche, Pfizer and Sarepta Therapeutics. LLB, AH, EW, CK, OH, and SFG indicated no potential conflicts of interest to disclose.
Figures



References
-
- Mendell J.R., Al-Zaidy S., Shell R., et al. Single-dose gene-replacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713–1722. - PubMed
-
- Day J.W., Finkel R.S., Chiriboga C.A., et al. Onasemnogene abeparvovec gene therapy for symptomatic infantile-onset spinal muscular atrophy in patients with two copies of SMN2 (STR1VE): an open-label, single-arm, multicentre, phase 3 trial. Lancet Neurol. 2021;20(4):284–293. - PubMed
-
- Mercuri E., Muntoni F., Baranello G., et al. Onasemnogene abeparvovec gene therapy for symptomatic infantile-onset spinal muscular atrophy type 1 (STR1VE-EU): an open-label, single-arm, multicentre, phase 3 trial. Lancet Neurol. 2021;20(10):832–841. - PubMed
-
- (FDA) USFDA . 2023. Onasemnogene abeparvovec-xioi (Zolgensma) STN: 125694.https://www.fda.gov/vaccines-blood-biologics/zolgensma [updated 10/18/2023]. Available from:
-
- Agency EM . 2023. Zolgensma (onasemongene abeparvovec) EMA/725800/2022.https://www.ema.europa.eu/en/documents/product-information/zolgensma-epa... [updated 17/03/2023]. Available from:
LinkOut - more resources
Full Text Sources
Miscellaneous
