

Effects of Pitavastatin on COVID-19 Incidence and Seriousness Among a Global Cohort of People With HIV
- PMID: 39435321
- PMCID: PMC11493083
- DOI: 10.1093/ofid/ofae574
Effects of Pitavastatin on COVID-19 Incidence and Seriousness Among a Global Cohort of People With HIV
Abstract
Background: Among people with HIV (PWH), COVID-19 is common and potentially severe. We leveraged REPRIEVE (Randomized Trial to Prevent Vascular Events in HIV) to assess the effects of statin therapy for cardiovascular disease prevention on COVID-19 outcomes (incidence and serious cases) among a global cohort of PWH.
Methods: COVID-19 data collection was implemented April 2020 to capture events from January 2020. COVID-19 was defined by positive test result or clinical diagnosis and serious COVID-19 according to the International Conference on Harmonisation definition. Among participants in follow-up on 1 January 2020, Cox proportional hazards modeling was used to estimate the hazard ratio (HR) of COVID-19 (pitavastatin/placebo), stratified by Global Burden of Disease region. Modification of statin effect following COVID-19 vaccination was evaluated via interaction with time-updated vaccination status.
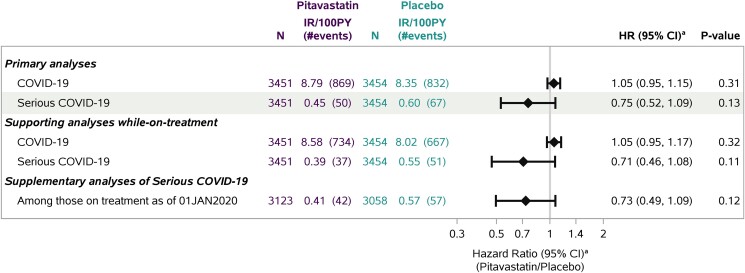
Results: Among 6905 PWH, 32% were natal female and 41% were Black or African American. The median age was 53 years and the 10-year atherosclerotic cardiovascular disease risk score 4.5%. Statin therapy did not reduce COVID-19 incidence (HR, 1.05; 95% CI, .95-1.15) but appeared to reduce incidence of serious COVID-19 (HR, 0.75; 95% CI, .52-1.09). Among 1701 PWH with COVID-19, the relative risk (pitavastatin/placebo) for serious COVID-19 was 0.73 (95% CI, .52-1.03). The treatment effect size for serious COVID-19 fell within the hypothesized range, but the 95% CI crossed 1 given fewer-than-anticipated cases (117 vs 200). Furthermore, 83% reported COVID-19 vaccination by end of study, with a strong protective effect on serious COVID-19 (HR, 0.27; 95% CI, .14-.53; P < .0001). A protective statin effect was observed prior to vaccination.
Conclusions: Among PWH, statin therapy had no effect on COVID-19 incidence but showed potential to reduce risk of serious COVID-19 prior to COVID-19 vaccination.
Clinical trials registration: NCT02344290 (ClinicalTrials.gov).
Keywords: COVID-19; HIV; PWH; REPRIEVE; statin.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. M. V. Z. reports grant support through her institution from the National Institutes of Health/National Institute of Allergy and Infectious Diseases (NIH/NIAID) and Gilead Sciences, Inc, relevant to the conduct of the study, as well as grants from NIH/NIAID and the NIH/National Heart, Lung, and Blood Institute (NHLBI); support for attending the Conference on Retroviruses and Opportunistic Infections and International Workshop for HIV and Women from conference organizing committee when abstract reviewer and/or speaker; and participation in a data and safety monitoring board for NIH funded studies, outside the submitted work. T. U. reports grants from NIH/NHLBI and Kowa Pharmaceuticals during the conduct of the study, as well as grants from NIH/NIAID and NIH/National Institute on Aging (NIA), outside the submitted work. C. J. F. reports research grants to his institution from Gilead Sciences, Merck, ViiV Healthcare and Moderna unrelated to this work. J. A. A. reports institutional research support for clinical trials from Emergent Biosolutions, Gilead Sciences, Glaxo Smith Kline, Janssen, Merck, Pfizer, Regeneron, and ViiV Healthcare; personal fees for advisory boards from Glaxo Smith Kline/ViiV and Merck; and participation on a data and safety monitoring board for Kintor Pharmaceuticals, all outside the submitted work. E. T. O. reports grant support from Gilead Sciences, ViiV Healthcare, and Janssen; consulting fees from ViiV Healthcare; and employment with ViiV Healthcare Medical Affairs, all outside the submitted work. C. D. M. reports institutional research support by Lilly and honoraria from ViiV Healthcare, Gilead Sciences, and Pfizer for advisory board membership, all outside the submitted work. J. S. C. reports consulting fees from Merck and Company and Resvirlogix, outside the submitted work. S. R. S. reports grant support through his institution from NIH/NIAID (T32 AI007387). K. M. E. reports grant support from NIH/NIA and Gilead Sciences, Inc; consulting fees paid to her institution from Gilead Sciences, Inc, ViiV Healthcare, and Janssen Therapeutics; and participation on an NIH data and safety monitoring board, all outside the submitted work. B. F. reports institutional research support from AstraZeneca, MedImmune, and MedTrace, as well as grants from NIH/NHLBI, all outside the submitted work. E. M. reports institutional research support from MSD and ViiV as well as honoraria for lectures or advisory boards from Gilead, Janssen, MDS, and ViiV. G. P. W. reports grant support through his institution from NIH/NIAID, NIH/National Institute of Diabetes and Digestive and Kidney Diseases, and Veterans Health Administration, all outside the submitted work. M. T. L. reports grant support through his institution from the NIH/NHLBI and Kowa Pharmaceuticals America for the conduct of the study. He also reports research support to his institution from the American Heart Association, AstraZeneca, Ionis, Johnson & Johnson Innovation, MedImmune, the National Academy of Medicine, the NIH/NHLBI, and the Risk Management Foundation of the Harvard Medical Institutions Incorporated, outside the submitted work. H. J. R. reports grants from Kowa Pharmaceuticals during the conduct of the study, as well as grants from NIH/NIAID, NIH/NHLBI, NIH/National Institute of Diabetes and Digestive and Kidney Diseases, and NIH/NIA, outside the submitted work. S. K. G. reports grant support through his institution from NIH, Kowa Pharmaceuticals America, Inc, Gilead Sciences, Inc, and ViiV Healthcare for the conduct of the study; personal fees from Theratechnologies and ViiV; and service on the Scientific Advisory Board of Marathon Asset Management, all outside the submitted work.
Figures
References
-
- Thornhill J, Orkin C, Cevik M. Estimating the global impact of coronavirus disease 2019 on people living with HIV. Curr Opin Infect Dis 2023; 36:20–5. - PubMed
Publication types
Associated data
Grants and funding
- UM1 AI068634/AI/NIAID NIH HHS/United States
- K24 AI157882/AI/NIAID NIH HHS/United States
- UL1 TR002384/TR/NCATS NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- T32 AI007387/AI/NIAID NIH HHS/United States
- UM1 AI069494/AI/NIAID NIH HHS/United States
- UG3 HL164285/HL/NHLBI NIH HHS/United States
- P30 DK040561/DK/NIDDK NIH HHS/United States
- U01 HL123336/HL/NHLBI NIH HHS/United States
- U24 HL164284/HL/NHLBI NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
