

Cardiovascular Risk Scores and Migraine Status
- PMID: 39436645
- PMCID: PMC11581481
- DOI: 10.1001/jamanetworkopen.2024.40577
Cardiovascular Risk Scores and Migraine Status
Abstract
Importance: A previous cohort study in the US found that women with higher cardiovascular risk were more likely to have a history of migraine but less likely to have active migraine. Extrapolating these results to men and European individuals is crucial to understanding the complex association between migraine activity status and vascular health in other populations.
Objective: To evaluate the association pattern between a cardiovascular risk score, the most recent European version of the Systematic Coronary Risk Evaluation 2 (SCORE2) risk estimation system, and migraine activity status in Dutch men and women.
Design, setting, and participants: The prospective population-based Lifelines cohort consists of community-dwelling adults residing in the northern part of the Netherlands. Individuals with a terminal illness, incapacitated individuals, including those with a severe mental illness, or who were unable to visit their general practitioner or complete the questionnaires were excluded from participation within Lifelines. Participants whose data on the cardiovascular risk scores and migraine status were complete were included in the analysis. Data on baseline characteristics were collected between November 1, 2006, to December 31, 2014. Cross-sectional and follow-up analyses were conducted within the prospective cohort. Questionnaires were sent approximately every 1.5 to 2.5 years, and the last self-reported migraine assessment took place between October 1, 2019, and January 31, 2021. Data were analyzed from March 1, 2022, to August 16, 2024.
Exposures: The SCORE2 is a sex-specific European cardiovascular risk score that includes age, cholesterol levels, smoking status, diabetes, and systolic blood pressure.
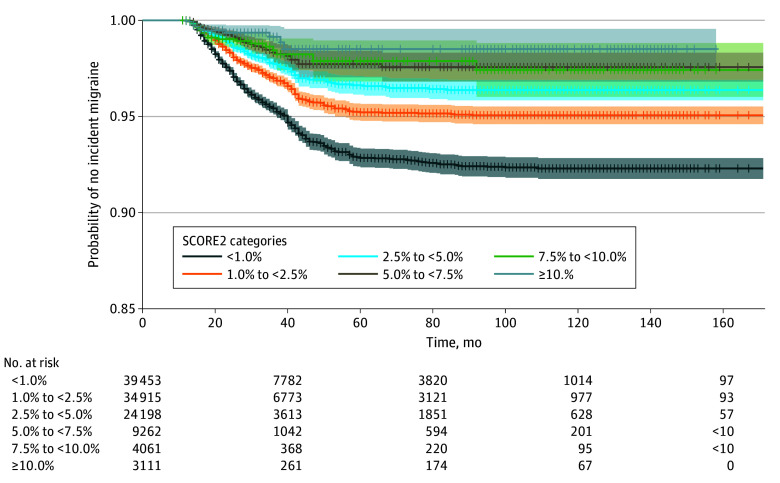
Main outcomes and measures: The primary outcome was the association pattern between cardiovascular risk scores and migraine activity status. SCORE2 risk scores were measured once at baseline; groups of the SCORE2 (<1.0%, 1.0% to <2.5%, 2.5% to <5.0%, 5.0% to <7.5%, 7.5% to <10.0%, and ≥10.0%) were created based on the sum of points of individual risk factors. Migraine activity status was assessed using self-reported questionnaires and classified as (1) prevalent (ie, migraine at baseline), (2) incident (ie, no migraine at baseline but migraine in ≥1 follow-up), and (3) none. To evaluate the influence of age, we conducted stratified analyses of the SCORE2 by age categories (<40, 40-49, and ≥50 years).
Results: The total study population consisted of 140 915 individuals at baseline with a mean (SD) age of 44.4 (12.7) years, of whom 58.5% were women. In total, 25 915 individuals (18.4% of the total population) had prevalent migraine and 2224 (1.9% of the 115 000 without prevalent migraine) had incident migraine. The odds of having prevalent and incident migraine, compared with individuals with a SCORE2 category of less than 1.0%, varied and decreased with increasing SCORE2 categories, with odds ratios (ORs) for prevalent migraine ranging from 0.93 (95% CI, 0.90-0.96) for a SCORE2 category of 1.0% to less than 2.5% to 0.43 (95% CI, 0.39-0.48) for a SCORE2 category of at least 10.0% and, for incident migraine, from 0.63 (95% CI, 0.57-0.69) for a SCORE2 category of 1.0% to less than 2.5% to 0.17 (95% CI, 0.10-0.27) for a SCORE2 category of at least 10.0%. A similar pattern was observed in both sexes but more profound in women. In women, ORs for prevalent migraine ranged from 1.21 (95% CI, 1.16-1.25) to 0.70 (95% CI, 0.58-0.83) (vs 1.19 [95% CI, 1.09-1.29] to 0.84 [95% CI, 0.72-0.99] in men) and, for incident migraine, 0.72 (95% CI, 0.64-0.80) to 0.20 (95% CI, 0.07-0.43) (vs 1.18 [95% CI, 0.92-1.52] to 0.44 [95% CI, 0.22-0.78] in men). Models with incident migraine as the outcome showed lower ORs across the ascending cardiovascular risk score categories. Age stratification suggested that the association between cardiovascular risk scores and migraine activity status were unlikely to be strongly influenced by age.
Conclusions and relevance: In this cohort study of community-dwelling Dutch adults, the odds of having prevalent or incident migraine decreased with increasing cardiovascular risk score categories. These results support the hypothesis that a relatively healthy cardiovascular system increases the probability of having active or developing migraine in the future, especially among women. Sex differences might play a pathophysiological role in the association between migraine activity and vascular health.
Conflict of interest statement
Figures
References
-
- Headache Classification Committee of the International Headache Society . The International Classification of Headache Disorders. 3rd ed. Cephalalgia; 2018;38(1):1-211. - PubMed
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211-1259. doi: 10.1016/S0140-6736(17)32154-2 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
