

Comorbidities confound metabolomics studies of human disease
- PMID: 39438584
- PMCID: PMC11496539
- DOI: 10.1038/s41598-024-75556-1
Comorbidities confound metabolomics studies of human disease
Abstract
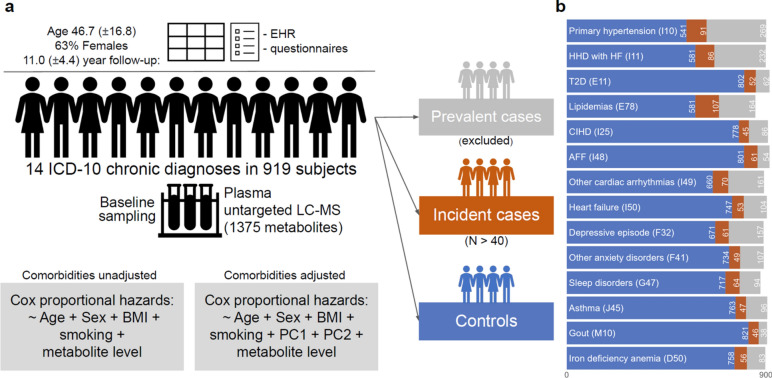
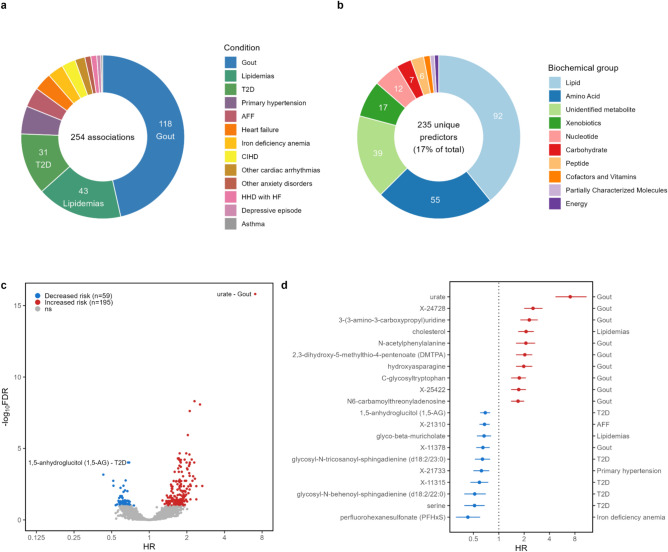
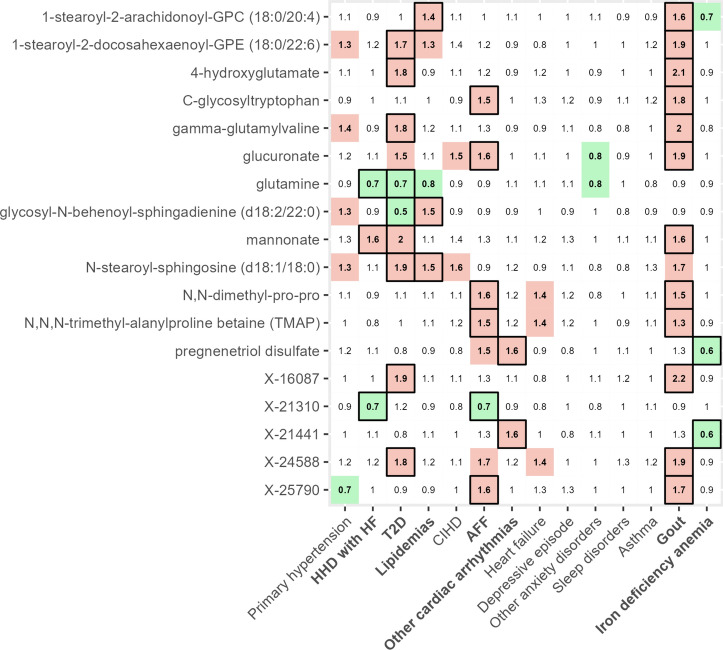
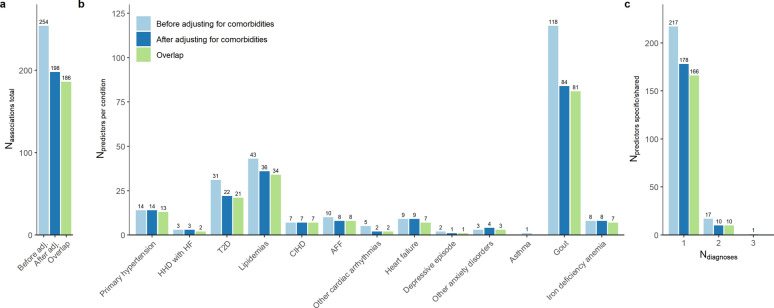
The co-occurrence of multiple chronic conditions, termed multimorbidity, presents an expanding global health challenge, demanding effective diagnostics and treatment strategies. Chronic ailments such as obesity, diabetes, and cardiovascular diseases have been linked to metabolites interacting between the host and microbiota. In this study, we investigated the impact of co-existing conditions on risk estimations for 1375 plasma metabolites in 919 individuals from population-based Estonian Biobank cohort using liquid chromatography mass spectrometry (LC-MS) method. We leveraged annually linked national electronic health records (EHRs) data to delineate comorbidities in incident cases and controls for the 14 common chronic conditions. Among the 254 associations observed across 13 chronic conditions, we primarily identified disease-specific risk factors (92%, 217/235), with most predictors (93%, 219/235) found to be related to the gut microbiome upon cross-referencing recent literature data. Accounting for comorbidities led to a reduction of common metabolite predictors across various conditions. In conclusion, our study underscores the potential of utilizing biobank-linked retrospective and prospective EHRs for the disease-specific profiling of diverse multifactorial chronic conditions.
Keywords: Biobank; Chronic disease; Comorbidities; Electronic health records; Metabolomics; Risk factors.
© 2024. The Author(s).
Conflict of interest statement
During the drafting of the manuscript, L.B. is an employee of BioMarin.
Figures
References
-
- Stanaway, J. D. et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease stu. Lancet392, 1923–1994. 10.1016/S0140-6736(18)32225-6 (2018). - PMC - PubMed
-
- Mars, N. et al. Polygenic and clinical risk scores and their impact on age at onset and prediction of cardiometabolic diseases and common cancers. Nat. Med.26, 549–557. 10.1038/S41591-020-0800-0 (2020). - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
