

Sodium-glucose cotransporter 2 inhibitors and cardiovascular events among patients with type 2 diabetes and low-to-normal body mass index: a nationwide cohort study
- PMID: 39438867
- PMCID: PMC11515712
- DOI: 10.1186/s12933-024-02478-7
Sodium-glucose cotransporter 2 inhibitors and cardiovascular events among patients with type 2 diabetes and low-to-normal body mass index: a nationwide cohort study
Abstract
Background: Patients with low-to-normal body mass index (BMI; < 25.0 kg/m2) were underrepresented in major randomized controlled trials on sodium-glucose cotransporter 2 (SGLT2) inhibitors for type 2 diabetes. The present study aims to investigate the effectiveness of SGLT2 inhibitors for cardiovascular outcomes among patients with type 2 diabetes and low-to-normal BMI, using finer stratification than previous trials.
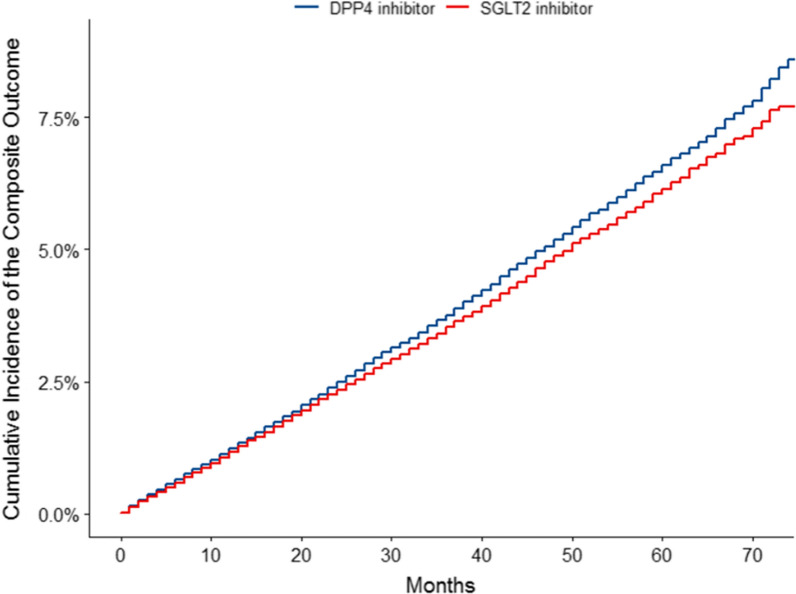
Methods: This cohort study with a target trial emulation framework was conducted using insurance claims and health screening records of more than 30 million working-age citizens in Japan acquired from April 1, 2015 to March 31, 2022. 139,783 new users of SGLT2 inhibitors matched to 139,783 users of dipeptidyl protease (DPP) 4 inhibitors with stratification by BMI category (< 20.0, 20.0-22.4, 22.5-24.9, 25.0-29.9, 30.0-34.9, and 35.0 ≤ kg/m2). The primary outcome was a composite of all-cause death, myocardial infarction, stroke, or heart failure. Secondary outcomes were the components of the primary outcome. Cox proportional hazard models were used to compare SGLT2 inhibitors with DPP4 inhibitors in the whole population and subgroups defined by the BMI category.
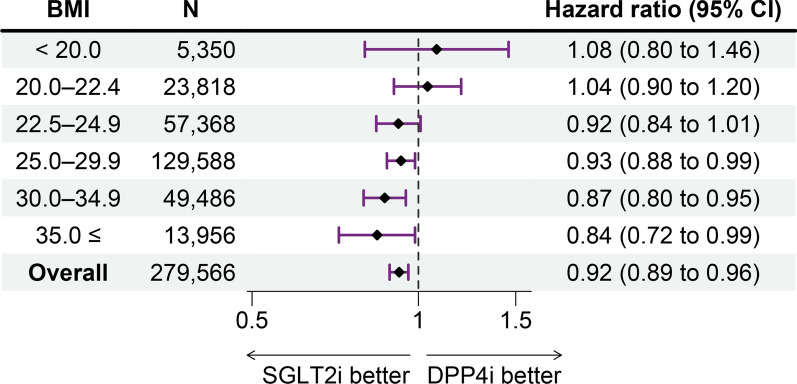
Results: Among participants, 17.3% (n = 48,377) were female and 31.0% (n = 86,536) had low-to-normal BMI (< 20.0 kg/m2, 1.9% [n = 5,350]; 20.0-22.4 kg/m2, 8.5% [n = 23,818]; and 22.5-24.9 kg/m2, 20.5% [n = 57,368]). Over a median follow-up of 24 months, the primary outcome occurred in 2.9% (n = 8,165) of participants. SGLT2 inhibitors were associated with a decreased incidence of the primary outcome in the whole population (HR [95%CI] = 0.92 [0.89 to 0.96]), but not in patients with low-to-normal BMI (< 20.0 kg/m2, HR [95%CI] = 1.08 [0.80 to 1.46]; 20.0-22.4 kg/m2, HR [95%CI] = 1.04 [0.90 to 1.20]; and 22.5-24.9 kg/m2, HR [95%CI] = 0.92 [0.84 to 1.01]).
Conclusions: The protective effect of SGLT2 inhibitors on cardiovascular events among patients with type 2 diabetes appeared to decrease with lower BMI and was not significant among patients with low-to-normal BMI (< 25.0 kg/m2). These findings suggest the importance of considering BMI when initiating SGLT2 inhibitors.
© 2024. The Author(s).
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure format (available on request from the corresponding author).
Figures


References
-
- Saeedi P, Salpea P, Karuranga S, et al. Mortality attributable to diabetes in 20–79 years old adults, 2019 estimates: results from the international diabetes federation diabetes atlas. Diabetes Res Clin Pract. 2020;162:108086. - PubMed
-
- Inoue K, Kondo N, Sato K, et al. Trends in cardiovascular risk factors by income among Japanese adults aged 30–49 years from 2017 to 2020: a nationwide longitudinal cohort study. Endocr Pract. 2023;29(3):185–92. - PubMed
-
- National academies of sciences, engineering, and medicine, division of behavioral and social sciences and education, committee on national statistics, et al. High and rising mortality rates among working-age adults. Becker T, Majmundar MK, Harris KM, editors. Washington, D.C., DC: National Academies Press; 2021. 596 p. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
