

Free fatty acids: independent predictors of long-term adverse cardiovascular outcomes in heart failure patients
- PMID: 39438940
- PMCID: PMC11495105
- DOI: 10.1186/s12944-024-02332-5
Free fatty acids: independent predictors of long-term adverse cardiovascular outcomes in heart failure patients
Abstract
Background: The association between plasma free fatty acid (FFA) and the outcomes in the heart failure (HF) patients remains unclear.
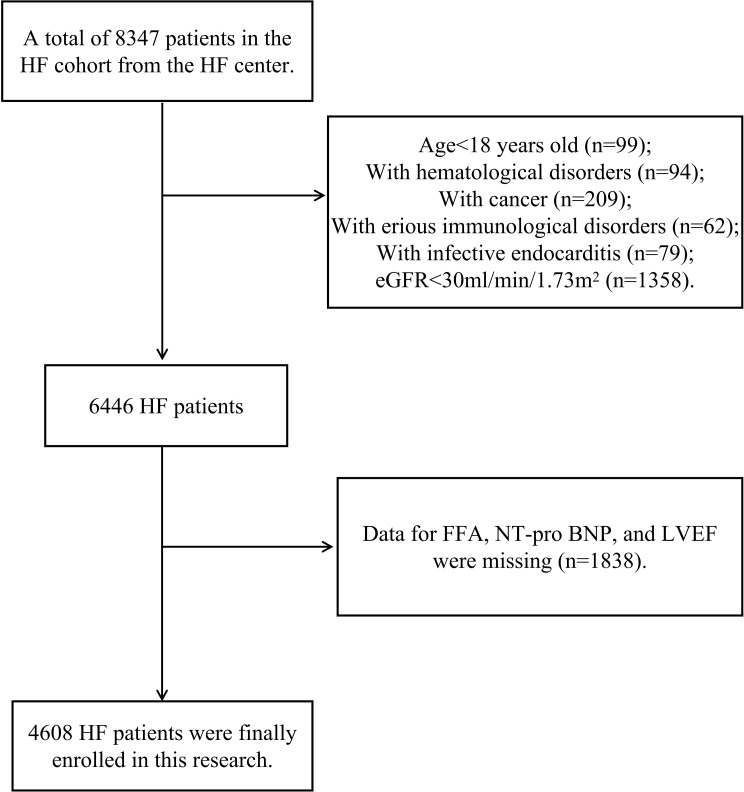
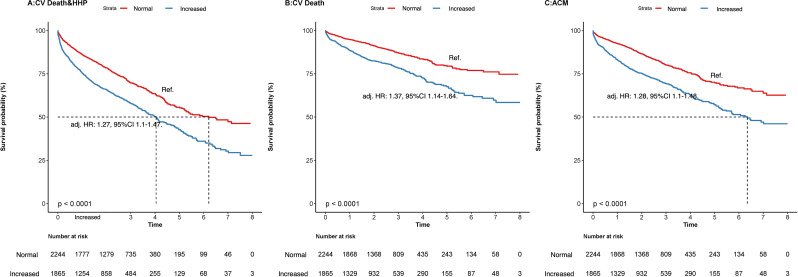
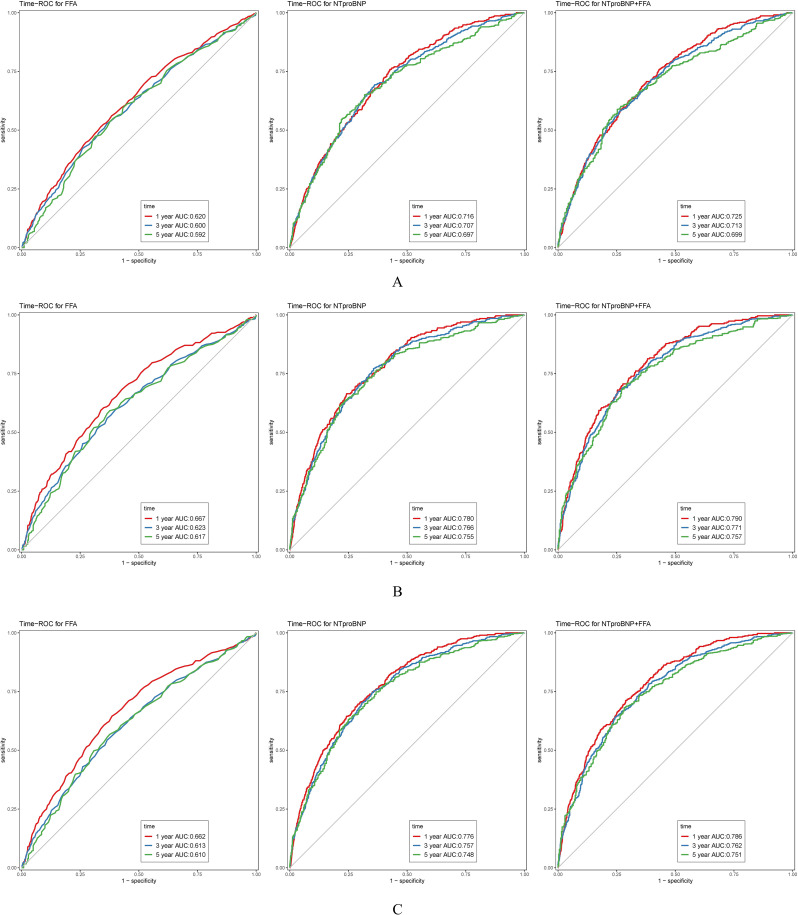
Methods: A cohort study among HF patients was performed. Plasma FFA was analyzed as both a continuous and a categorical variable (grouped by tertiles) to assess its association with composite cardiovascular (CV) death and HF hospitalization (CV death & HHP), CV death alone, and all-cause mortality (ACM) using Cox regression models. Subgroup analyses of HF patients with preserved ejection fraction (HFpEF) and mildly reduced/reduced ejection fraction (HFmrEF/HFrEF) were performed. This work also assessed the effectiveness of combining FFA and NT-pro BNP biomarkers for risk stratification by calculating the concordance index (C-index).
Results: Among the 4,109 HF patients, FFA levels exceeding 0.4-0.42 mmol/L were associated with increased risks of the three outcomes. Patients in the highest FFA tertile faced greater risks than those in the lowest tertile. Adjusted hazard ratios were 1.32 (95% CI: 1.11-1.58) for CV death & HHP, 1.45 (95% CI: 1.16-1.82) for CV death, and 1.39 (95% CI: 1.15-1.68) for ACM, with a maximum follow-up of 8 years (median: 25 months). Subgroup analyses revealed that elevated FFA levels consistently predicted worse outcomes in both HFmrEF/HFrEF and HFpEF patients. The C-index for predicting outcomes was significantly greater when NT-pro BNP and FFA were combined than when NT-pro BNP was used alone (P < 0.01).
Conclusion: Increased plasma FFA concentrations were independently associated with greater risks of CV death & HHP, CV death, and ACM among HF patients, irrespective of the ejection fraction. The combination of FFA and NT-pro BNP biomarkers significantly improved risk stratification in HF patients.
Keywords: Adverse cardiovascular outcomes; All-cause mortality; Free fatty acids; Heart failure; Long-term follow-up.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Doehner W, Frenneaux M, Anker SD. Metabolic impairment in heart failure: the myocardial and systemic perspective. J Am Coll Cardiol. 2014;64(13):1388–400. - PubMed
-
- Carlsson M, Wessman Y, Almgren P, et al. High levels of nonesterified fatty acids are associated with increased familial risk of cardiovascular disease. Arterioscler Thromb Vasc Biol. 2000;20(6):1588–94. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
