

The New Zealand Parkinson's progression programme
- PMID: 39439968
- PMCID: PMC11459764
- DOI: 10.1080/03036758.2022.2111448
The New Zealand Parkinson's progression programme
Abstract
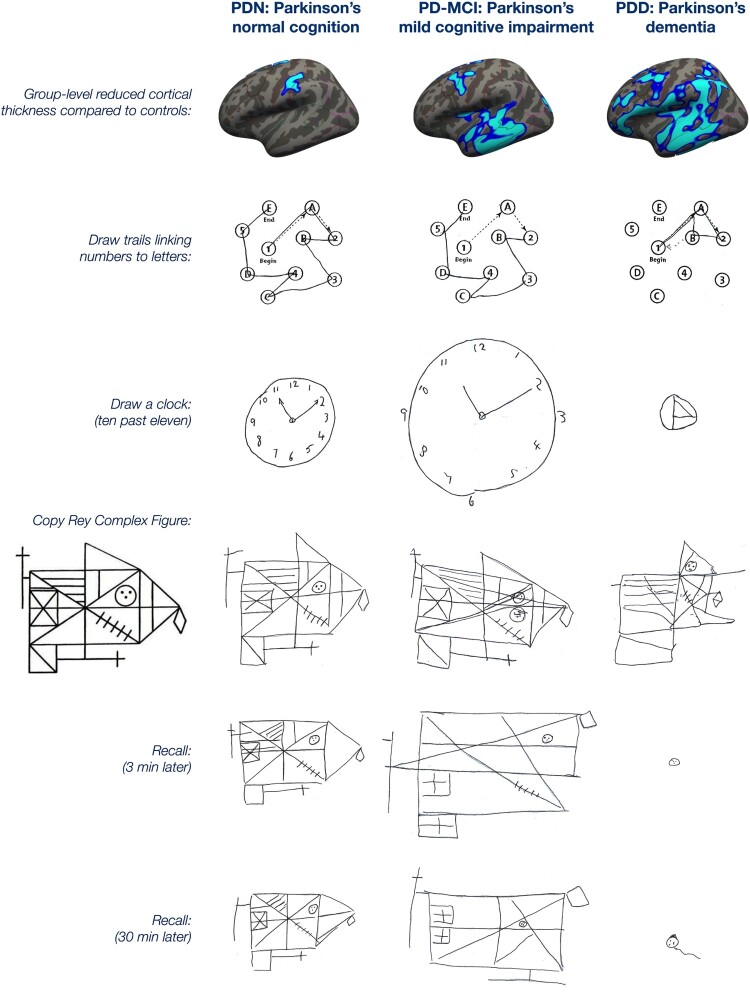
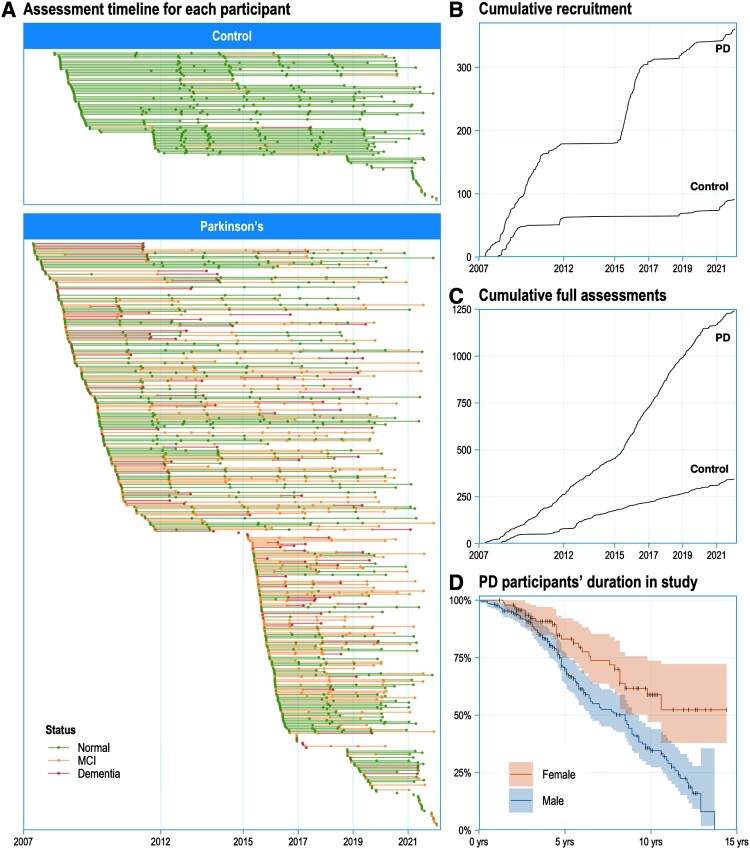
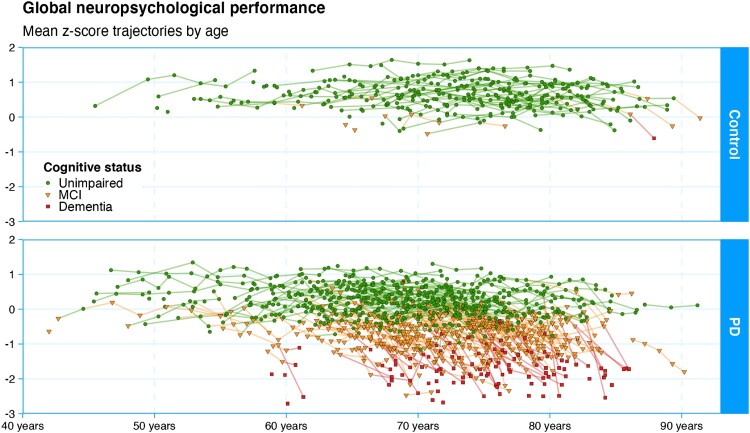
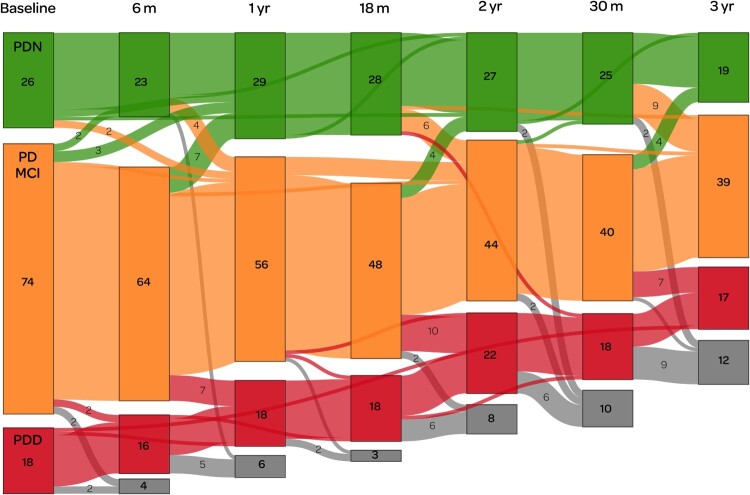
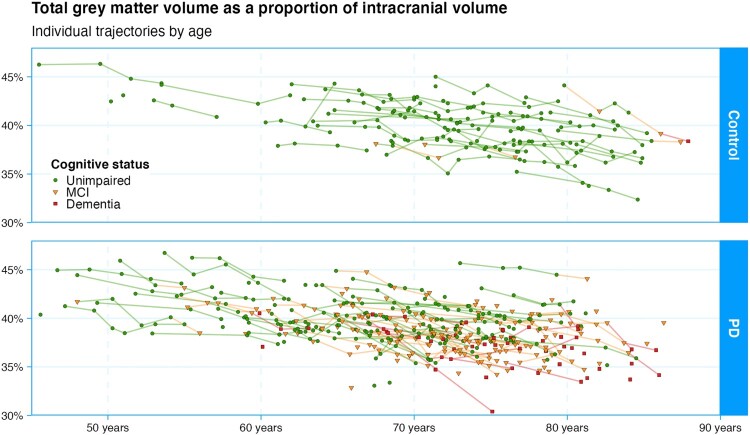
We describe the New Zealand Parkinson's Progression Programme (NZP3), its goals, findings, and future plans. To date, 354 people with Parkinson's disease and 89 healthy older controls have participated over a 14-year period. A major focus of the programme has been the characterisation of current cognitive impairment, and the identification of biomarkers for its future emergence in people with Parkinson's. The programme has made significant contributions to the concept of mild cognitive impairment (MCI) in Parkinson's and the development and validation of standardised criteria for it. Brain imaging, both MRI and PET, has also been a focus, showing associations between increasing brain pathology and declining cognitive function. Additional biomarkers such as genetics, fluid biomarkers, eye movement, speech, and quantitative electroencephalography (EEG) are also under investigation. The programme has become a platform supporting many other avenues of research, from investigating the personal impacts of caregiver burden through to national-level epidemiology. To date, the programme has led to multiple journal publications and 17 completed and 9 ongoing PhDs, and many other postgraduate theses. It has led to the development of a skilled core of early-career through to senior researchers and clinicians. We discuss the future directions for the programme.
Keywords: Parkinson’s disease; cognitive impairment; dementia; longitudinal assessment; neuropsychology.
© 2022 The Royal Society of New Zealand.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Almuqbel M, Melzer TR, Myall DJ, MacAskill MR, Pitcher TL, Livingston L, Wood K-LL, Keenan RJ, Dalrymple-Alford JC, Anderson TJ.. 2016. Metabolite ratios in the posterior cingulate cortex do not track cognitive decline in Parkinson’s disease in a clinical setting. Parkinsonism and Related Disorders. 22:54–61. doi: 10.1016/j.parkreldis.2015.11.008. - DOI - PubMed
-
- Anderson TJ, Ewer TC, Gilchrist NL, Donaldson IM.. 1992. Trial of Sinemet CR4 in patients with Parkinson’s disease. New Zealand Medical Journal. 105(929):81–82. - PubMed
-
- Anderson TJ, Jenkins IH, Brooks DJ, Hawken MB, Frackowiak RSJ, Kennard C.. 1994. Cortical control of saccades and fixation in man: a PET study. Brain. 117:1073–1084. - PubMed
LinkOut - more resources
Full Text Sources