

Mid-jejunal diverticulitis with closed-loop bowel obstruction, strangulation, and contained perforation
- PMID: 39440345
- PMCID: PMC11493754
- DOI: 10.1002/ccr3.9489
Mid-jejunal diverticulitis with closed-loop bowel obstruction, strangulation, and contained perforation
Abstract
Key clinical message: Closed-loop bowel obstruction and contained perforation secondary to acute on chronic jejunal diverticulitis is rare and should be included in the differential diagnosis of acute abdomen. The association between polymyalgia rheumatica and diverticular disease requires further research but may prompt clinicians to consider appropriate therapies in patients with both diseases.
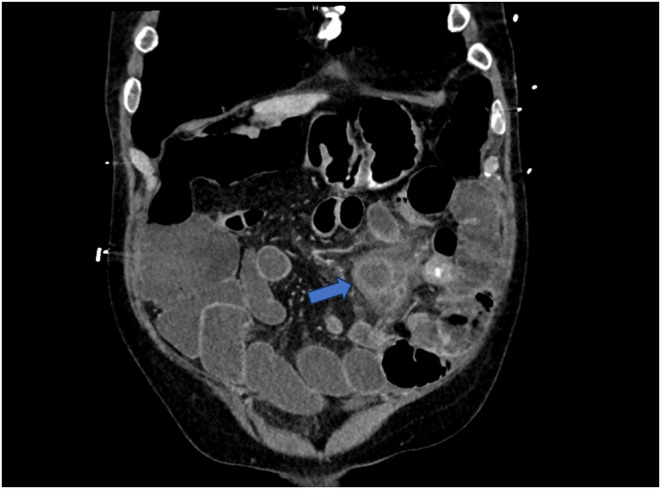
Abstract: Jejunal diverticulosis is a sac-like outpouching of the intestinal wall that can cause complications such as diverticulitis, obstruction, abscess, perforation, or fistula formation. Complicated jejunal diverticulosis may present with acute abdomen and nonspecific symptoms which can lead to misdiagnosis and delayed treatment. A 76-year-old male with a remote history of polymyalgia rheumatica (PMR) presented with sudden onset abdominal pain, fever, nausea, vomiting, and inability to pass flatus. Physical exam revealed a distended and diffusely tender abdomen with signs of peritonitis. Laboratory test results were significant for neutrophil-dominant leukocytosis and elevated inflammatory markers. CT scan of the abdomen with IV contrast revealed a contained perforation and a closed-loop small bowel obstruction in the mid-abdomen. The patient underwent emergent exploratory laparotomy and resection of 100 cm of mid-jejunum which was found to have numerous diverticula surrounding the closed-loop obstruction and contained perforation. Pathology findings showed evidence of acute on chronic jejunal diverticulitis. Jejunal diverticulosis with complications may present with an acute abdomen and peritonitis. Closed-loop bowel obstruction and contained perforation secondary to acute on chronic jejunal diverticulitis is uncommonly thought of and should be considered in the differential diagnosis. Additionally, the association between PMR and diverticular disease is notable. While the patient had a remote history but no active PMR on presentation, studies suggest a possible association between gut inflammation and rheumatologic disease. This association should prompt clinicians to consider appropriate therapies and bear in mind the potential risk for diverticular perforation if glucocorticoids are given to treat PMR. Jejunal diverticulosis with multiple complications such as closed-loop bowel obstruction and contained perforation secondary to acute on chronic jejunal diverticulitis is rare and may present with an acute abdomen and nonspecific symptoms. Including rare pathologies as such in the differential diagnosis may prevent misdiagnosis and delayed treatment. While further investigation is needed, the association between diverticulosis and PMR is noteworthy as patients who present with both diseases would require mindful management due to the potential risk of diverticular perforation after treatment with steroids.
Keywords: diverticular diseases; diverticulitis; intestinal obstruction; intestinal perforation; jejunal diseases; polymyalgia rheumatica.
© 2024 The Author(s). Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures









References
LinkOut - more resources
Full Text Sources
