

Procoagulant platelet activation promotes venous thrombosis
- PMID: 39440970
- PMCID: PMC11662225
- DOI: 10.1182/blood.2024025476
Procoagulant platelet activation promotes venous thrombosis
Abstract
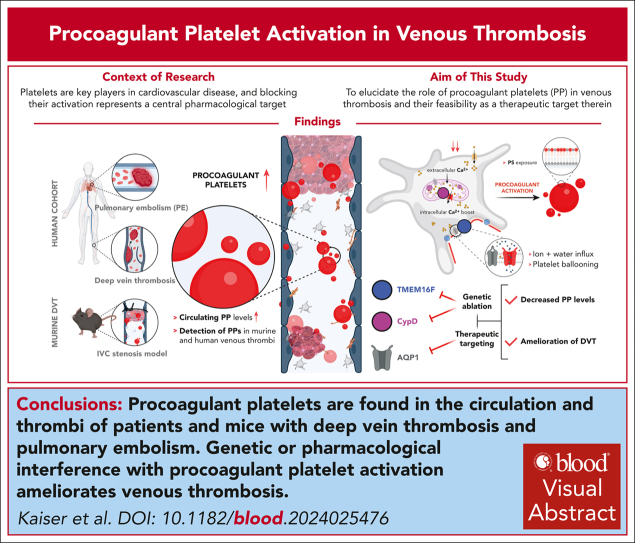
Platelets are key players in cardiovascular disease, and platelet aggregation represents a central pharmacologic target, particularly in secondary prevention. However, inhibition of adenosine diphosphate and thromboxane signaling has low efficacy in preventing venous thromboembolism, necessitating the inhibition of the plasmatic coagulation cascade in this disease entity. Anticoagulation carries a significantly higher risk of bleeding complications, highlighting the need of alternative therapeutic approaches. We hypothesized that procoagulant activation (PA) of platelets promotes venous thrombus formation and that targeting PA could alleviate venous thrombosis. Here, we found elevated levels of procoagulant platelets in the circulation and in thrombi of patients with deep vein thrombosis (DVT) and pulmonary embolism, and in mice developing DVT following inferior vena cava stenosis. Furthermore, we detected PA of recruited platelets within murine venous thrombi and human pulmonary emboli. Mice with platelet-specific deficiency in central pathways of PA-cyclophilin D and transmembrane protein 16F-were more resistant toward low flow-induced venous thrombosis. Finally, we found that a clinically approved carbonic anhydrase inhibitor, methazolamide, reduced platelet procoagulant activity and alleviated murine thrombus formation without affecting trauma-associated hemostasis. These findings identify an essential role of platelet procoagulant function in venous thrombosis and delineate novel pharmacologic strategies targeting platelets in the prevention of venous thromboembolism.
© 2024 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: T.B. and J.K. have an exclusive licensing agreement with BioLegend, Inc, for the commercialization of mC1-multimer. The remaining authors declare no competing financial interests.
Figures



References
-
- Martin SS, Aday AW, Almarzooq ZI, et al. 2024 Heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2024;149(8):e347–e913. - PubMed
-
- Jackson SP. Arterial thrombosis--insidious, unpredictable and deadly. Nat Med. 2011;17(11):1423–1436. - PubMed
-
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS) Eur Heart J. 2020;41(4):543–603. - PubMed
-
- O’Toole RV, Stein DM, O’Hara NN, et al. Major Extremity Trauma Research Consortium (METRC). Aspirin or low-molecular-weight heparin for thromboprophylaxis after a fracture. N Engl J Med. 2023;388(3):203–213. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
