

Ventilation strategies in cardiogenic shock: insights from the FRENSHOCK observational registry
- PMID: 39441346
- PMCID: PMC12460561
- DOI: 10.1007/s00392-024-02551-x
Ventilation strategies in cardiogenic shock: insights from the FRENSHOCK observational registry
Abstract
Background: Despite scarce data, invasive mechanical ventilation (MV) is widely suggested as first-line ventilatory support in cardiogenic shock (CS) patients. We assessed the real-life use of different ventilation strategies in CS and their influence on short and mid-term prognosis.
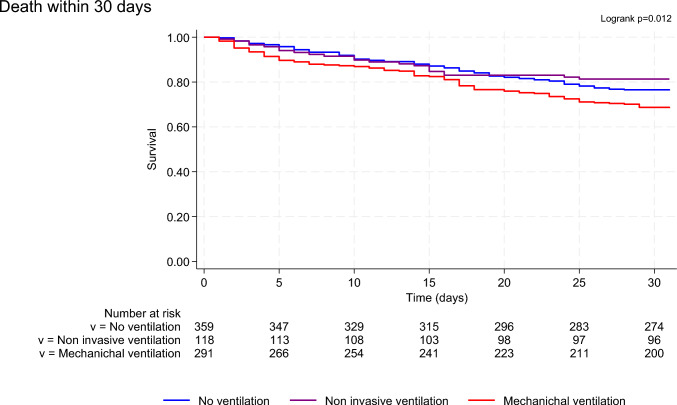
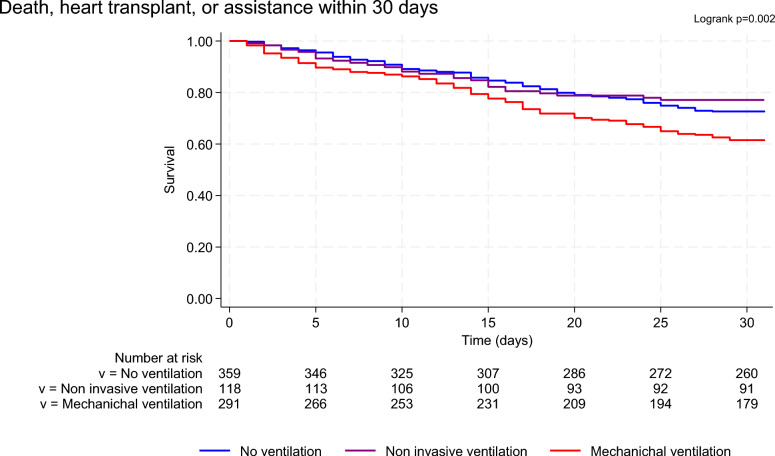
Methods: FRENSHOCK was a prospective registry including 772 CS patients from 49 centers in France. Patients were categorized into three groups according to the ventilatory supports during hospitalization: no mechanical ventilation group (NV), non-invasive ventilation alone group (NIV), and invasive mechanical ventilation group (MV). We compared clinical characteristics, management, and occurrence of death and major adverse event (MAE) (death, heart transplantation or ventricular assist device) at 30 days and 1 year between the three groups.
Results: Seven hundred sixty-eight patients were included in this analysis. Mean age was 66 years and 71% were men. Among them, 359 did not receive any ventilatory support (46.7%), 118 only NIV (15.4%), and 291 MV (37.9%). MV patients presented more severe CS with more skin mottling, higher lactate levels, and higher use of vasoactive drugs and mechanical circulatory support. MV was associated with higher mortality and MAE at 30 days (HR 1.41 [1.05-1.90] and 1.52 [1.16-1.99] vs NV). No difference in mortality (HR 0.79 [0.49-1.26]) or MAE (HR 0.83 [0.54-1.27]) was found between NIV patients and NV patients. Similar results were found at 1-year follow-up.
Conclusions: Our study suggests that using NIV is safe in selected patients with less profound CS and no other MV indication. NCT02703038.
Keywords: Cardiogenic shock; Mechanical ventilation; Mortality; Non-invasive ventilation; Prognosis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare that they have no conflict of interest.
Figures
References
-
- Van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK (2017) Contemporary management of cardiogenic shock: a scientific statement from the american heart association. Circulation 136(16):e232–e268 - PubMed
-
- Zeymer U, Vogt A, Zahn R, Weber MA, Tebbe U, Gottwik M (2004) Predictors of in-hospital mortality in 1333 patients with acute myocardial infarction complicated by cardiogenic shock treated with primary percutaneous coronary intervention (PCI): results of the primary PCI registry of the Arbeitsgemeinschaft Leitende Kardiologische Krankenhausarzte (ALKK). Eur Heart J 25(4):322–328 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
