

Visualization of cortical neoangiogenesis after combined revascularization surgery in moyamoya disease using silent MRA
- PMID: 39441413
- PMCID: PMC11893653
- DOI: 10.1007/s00234-024-03486-w
Visualization of cortical neoangiogenesis after combined revascularization surgery in moyamoya disease using silent MRA
Abstract
Purpose: To investigate postsurgical indirect cortical neoangiogenesis in patients with moyamoya disease (MMD) using silent magnetic resonance angiography (MRA).
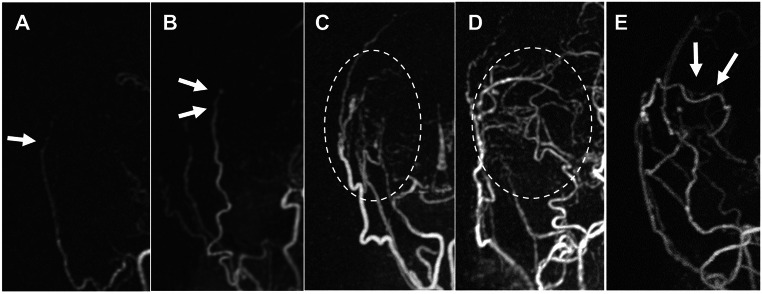
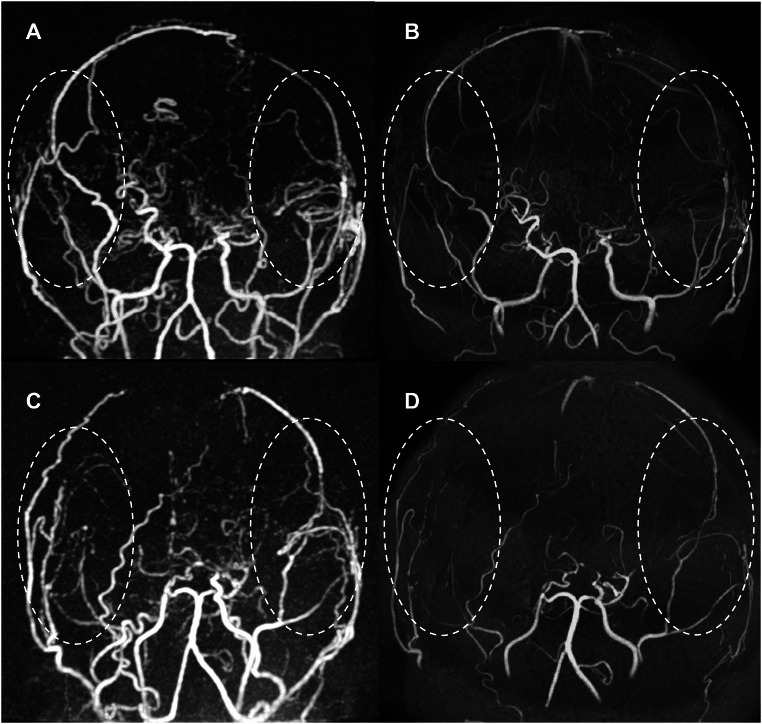
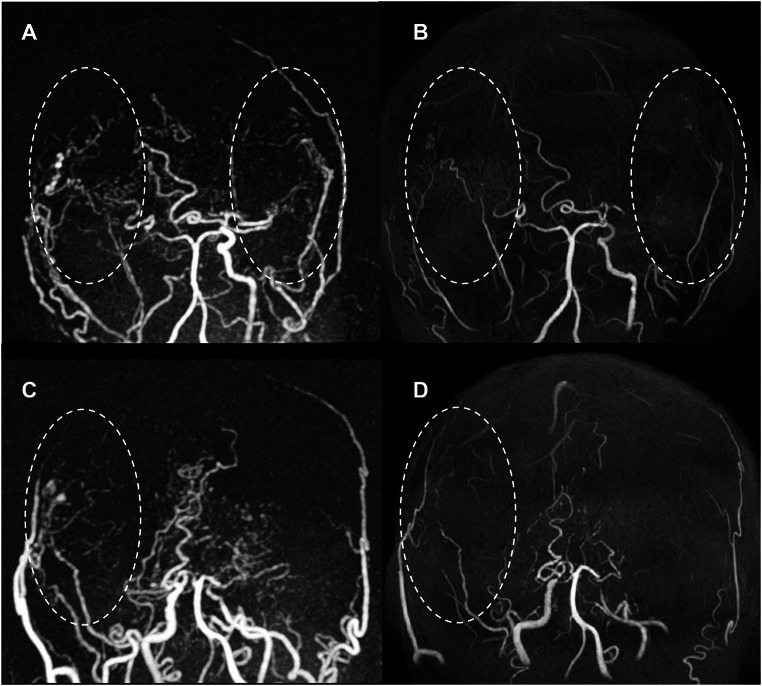
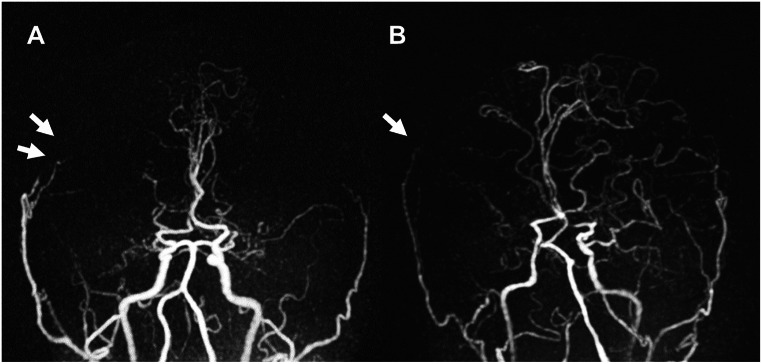
Methods: We studied 44 patients with MMD (63 hemispheres) who were previously revascularized with combined bypass surgery (23 and 40 hemispheres in pediatric and adult patients, respectively). They underwent follow-up for postoperative bypass patency using time-of-flight (TOF)-MRA and silent MRA between January 2022 and December 2023. The mean duration from surgery to MRA was 8.5 years (range, 1.2-22.3 years). Two observers independently rated the revascularization as follows: 0 (near-complete signal loss or no signal); 1, poor (slightly visible donor arteries); 2, good (acceptable revascularization around the brain surface); and 3, excellent (good quality of revascularization with perfusion from the cortical surface into the middle cerebral artery).
Results: Silent MRA visualized indirect bypass significantly better than TOF-MRA (2.6 ± 0.7 and 1.4 ± 0.8) (P < 0.01). In silent MRA, the mean score of indirect bypass was significantly higher than that of direct bypass (2.6 ± 0.7 and 1.7 ± 1.0; P < 0.01) and indicated good indirect bypass development in both children and adults (91.3% and 85.0%; score ≥ 2). Children exhibited a higher rate of excellent indirect bypass patency than adults (73.9% and 55.0%; score 3). Poor bypass development in indirect bypass (8 hemispheres, mean age: 35.5 ± 17.5 years, mean follow-up period: 11.3 years) was significantly observed in male patients (P < 0.01).
Conclusion: Silent MRA enables better precision in postsurgical visualization of indirect cortical neoangiogenesis during long-term follow-up and reveals indirect bypass development even in adult patients.
Keywords: Cortical neoangiogenesis; Indirect bypass; Moyamoya disease; Silent MRA; UTE-MRA.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: This study was approved by the Ethics Committee of Niigata University Medical and Dental Hospital (approval number: 2019 − 0187). Informed consent: Patient consent was waived because of the retrospective nature of the study and the analysis used anonymous clinical data. Disclosures: None.
Figures
References
-
- Suzuki J, Takaku A (1969) Cerebrovascular moyamoya disease. Disease showing abnormal net-like vessels in base of brain. Arch Neurol 20:288–299. 10.1001/archneur.1969.00480090076012 - PubMed
-
- Kuroda S, Houkin K (2008) Moyamoya disease: current concepts and future perspectives. Lancet Neurol 7:1056–1066. 10.1016/S1474-4422(08)70240-0 - PubMed
-
- Macyszyn L, Attiah M, Ma TS, Ali Z, Faught R, Hossain A, Man K, Patel H, Sobota R, Zager EL, Stein SC (2017) Direct versus indirect revascularization procedures for moyamoya disease: a comparative effectiveness study. J Neurosurg 126:1523–1529. 10.3171/2015.8.JNS15504 - PubMed
-
- Park S-E, Kim J-S, Park EK, Shim K-W, Kim D-S (2018) Direct versus indirect revascularization in the treatment of moyamoya disease. J Neurosurg 129:480–489. 10.3171/2017.5.JNS17353 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
