

Carcinoid heart disease in patients with advanced small-intestinal neuroendocrine tumors and carcinoid syndrome: a retrospective experience from two European referral centers
- PMID: 39442478
- PMCID: PMC11538955
- DOI: 10.1016/j.esmoop.2024.103959
Carcinoid heart disease in patients with advanced small-intestinal neuroendocrine tumors and carcinoid syndrome: a retrospective experience from two European referral centers
Abstract
Background: Up to 50% of patients with advanced small-intestinal neuroendocrine tumors (SI-NETs) and carcinoid syndrome (CS) develop carcinoid heart disease (CHD). However, the true frequency and prognostic markers for CHD in CS are lacking. We described the real-world management of patients in two NET referral centers in this clinical context and relationships between clinical features, including CHD and overall survival (OS).
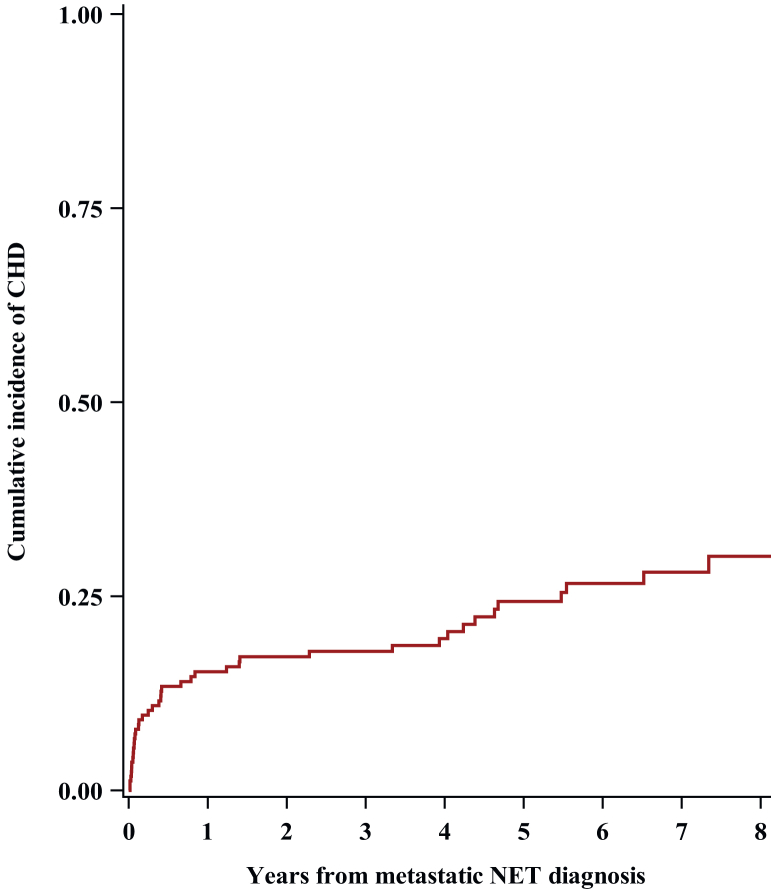
Patients and methods: This is a retrospective analysis of patients with stage IV SI-NET and CS, treated at the European Institute of Oncology in Milan and Uppsala University in Sweden between 2015 and 2021. CHD was defined as at least one moderate right-sided heart valve defect. Median OS and cumulative incidence of CHD were estimated from the diagnosis of metastatic disease, and the association between clinical parameters with both OS and occurrence of CHD was evaluated.
Results: We included 165 patients, with 97% having low-intermediate-grade SI-NETs and 86% having synchronous liver metastases. Ninety-eight patients (59%) became refractory to full label dose of somatostatin analogues and 25% developed a CHD. At CHD diagnosis, baseline urine 5-hydroxyindoleacetic acid (24-h u5-HIAA) value and plasma N-terminal pro-brain natriuretic peptide (NT-proBNP) value were known in 76% of patients. Moderate-to-severe tricuspid insufficiency was the most common alteration of CHD. Prognosis was significantly impaired by CHD (multivariable hazard ratio for OS = 2.85, P < 0.001). The median OS from the CHD diagnosis was 4.5 years [95% confidence interval (CI) 2.1-7.2 years], and the 5-year survival rate was 34% (95% CI 13% to 57%).
Conclusions: In our study population of SI-NET patients with CS, more than half had a refractory carcinoid syndrome (RCS) and one-quarter developed a CHD, with a negative impact on OS. Therefore, it is recommended to screen and monitor patients with CS for CHD, ideally with a combination of u5-HIAA, NT-proBNP values, and echocardiography at CS baseline, preferably in NET referral centers.
Keywords: carcinoid heart disease; carcinoid syndrome; neuroendocrine tumor; small intestinal.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Sorbye H., Grande E., Pavel M., et al. European Neuroendocrine Tumor Society (ENETS) 2023 guidance paper for digestive neuroendocrine carcinoma. J Neuroendocrinol. 2023;35(3):e13249. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
