

Intensive chemotherapy versus standard chemotherapy among patients with high risk, operable, triple negative breast cancer based on integrated mRNA-lncRNA signature (BCTOP-T-A01): randomised, multicentre, phase 3 trial
- PMID: 39442958
- PMCID: PMC11497771
- DOI: 10.1136/bmj-2024-079603
Intensive chemotherapy versus standard chemotherapy among patients with high risk, operable, triple negative breast cancer based on integrated mRNA-lncRNA signature (BCTOP-T-A01): randomised, multicentre, phase 3 trial
Abstract
Objective: To evaluate the feasibility of using a multigene signature to tailor individualised adjuvant therapy for patients with operable triple negative breast cancer.
Design: Randomised, multicentre, open label, phase 3 trial.
Setting: 7 cancer centres in China between 3 January 2016 and 17 July 2023.
Participants: Female patients aged 18-70 years with early triple negative breast cancer after definitive surgery.
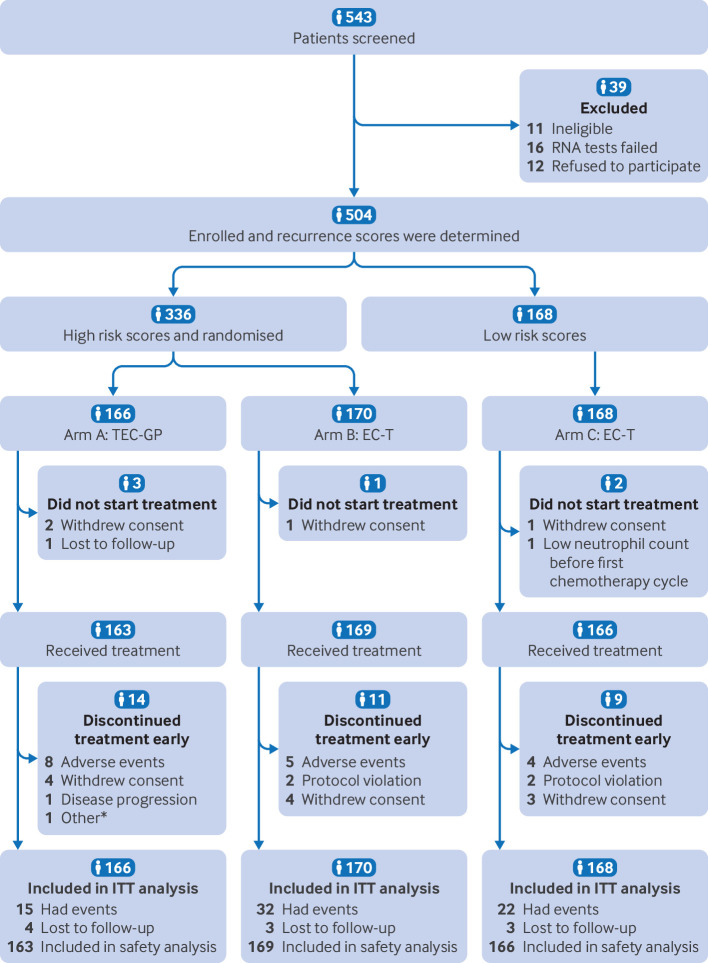
Interventions: After risk stratification using the integrated signature, patients at high risk were randomised (1:1) to receive an intensive adjuvant treatment comprising four cycles of docetaxel, epirubicin, and cyclophosphamide followed by four cycles of gemcitabine and cisplatin (arm A; n=166) or a standard treatment of four cycles of epirubicin and cyclophosphamide followed by four cycles of docetaxel (arm B; n=170). Patients at low risk received the same adjuvant chemotherapy as arm B (arm C; n=168).
Main outcome measures: The primary endpoint was disease-free survival in the intention-to-treat analysis for arm A versus arm B. Secondary endpoints included disease-free survival for arm C versus arm B, recurrence-free survival, overall survival, and safety.
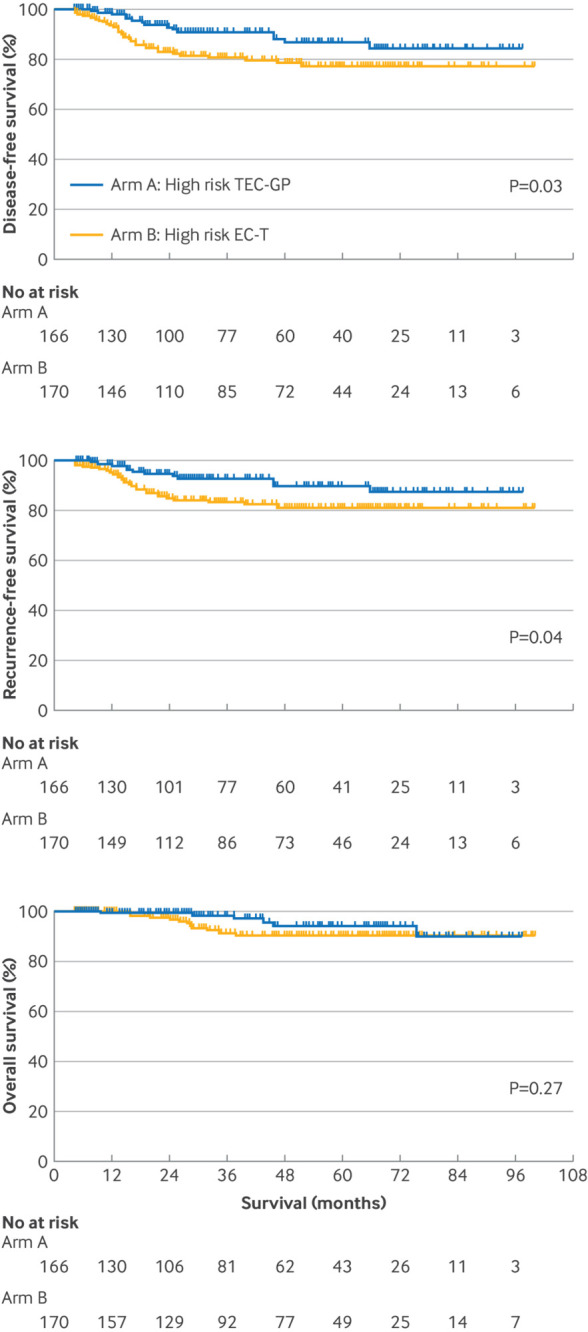
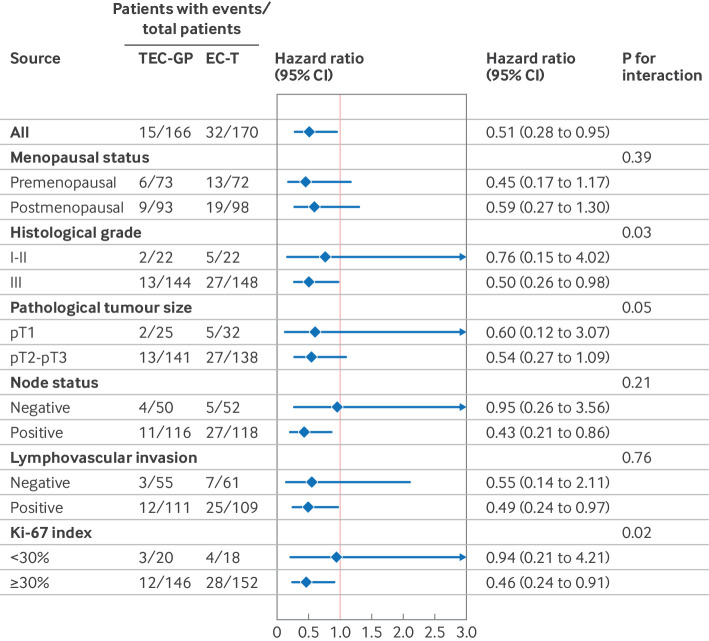
Results: Among the 504 enrolled patients, 498 received study treatment. At a median follow-up of 45.1 months, the three year disease-free survival rate was 90.9% for patients in arm A and 80.6% for patients in arm B (hazard ratio 0.51, 95% confidence interval (CI) 0.28 to 0.95; P=0.03). The three year recurrence-free survival rate was 92.6% in arm A and 83.2% in arm B (hazard ratio 0.50, 95% CI 0.25 to 0.98; P=0.04). The three year overall survival rate was 98.2% in arm A and 91.3% in arm B (hazard ratio 0.58, 95% CI 0.22 to 1.54; P=0.27). The rates of disease-free survival (three year disease-free survival 90.1% v 80.6%; hazard ratio 0.57, 95% CI 0.33 to 0.98; P=0.04), recurrence-free survival (three year recurrence-free survival 94.5% v 83.2%; 0.42, 0.22 to 0.81; P=0.007), and overall survival (three year overall survival 100% v 91.3%; 0.14, 0.03 to 0.61; P=0.002) were significantly higher in patients in arm C than in those in arm B with the same chemotherapy regimen. The incidence of grade 3-4 treatment related adverse events were 64% (105/163), 51% (86/169), and 54% (90/166) for arms A, B, and C, respectively. No treatment related deaths occurred.
Conclusions: The multigene signature showed potential for tailoring adjuvant chemotherapy for patients with operable triple negative breast cancer. Intensive regimens incorporating gemcitabine and cisplatin into anthracycline/taxane based therapy significantly improved disease-free survival with manageable toxicity.
Trial registration: ClinicalTrials.gov NCT02641847.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare: support from the National Key Research and Development Project of China, National Natural Science Foundation of China, Science and Technology Commission of Shanghai Municipality, Shanghai Key Laboratory of Breast Cancer, SHDC Municipal Project for Developing Emerging and Frontier Technology in Shanghai Hospitals, and CSPC Pharmaceutical Co Ltd, Shijiazhuang, China, for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical