

Adjudication of Hospitalizations and Deaths in the IRONMAN Trial of Intravenous Iron for Heart Failure
- PMID: 39443013
- PMCID: PMC11496827
- DOI: 10.1016/j.jacc.2024.08.052
Adjudication of Hospitalizations and Deaths in the IRONMAN Trial of Intravenous Iron for Heart Failure
Abstract
Background: Patients with heart failure and iron deficiency have diverse causes for hospitalization and death that might be affected by iron repletion.
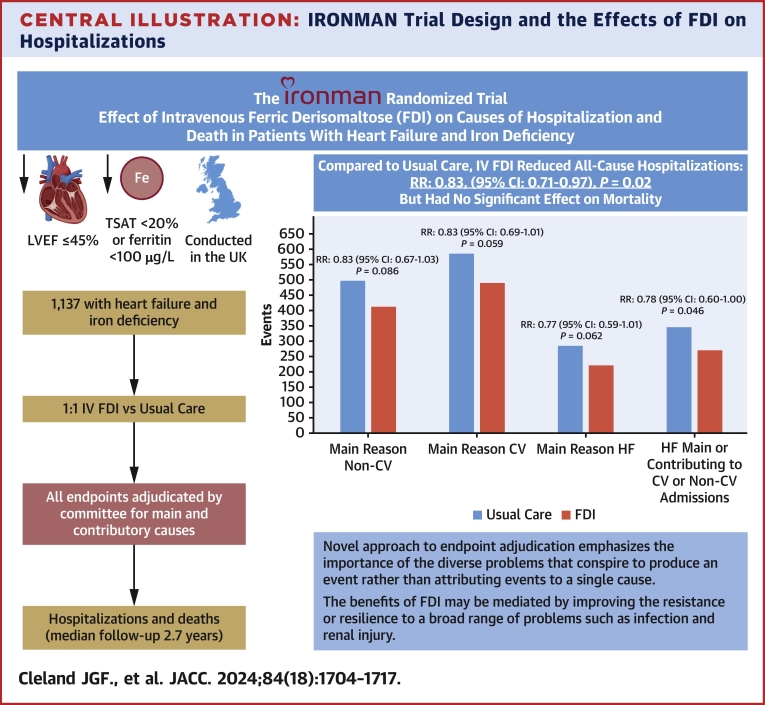
Objectives: The purpose of this study was to explore causes of hospitalizations and deaths in a randomized trial (IRONMAN) of heart failure comparing intravenous ferric derisomaltose (FDI) (n = 568) and usual care (n = 569).
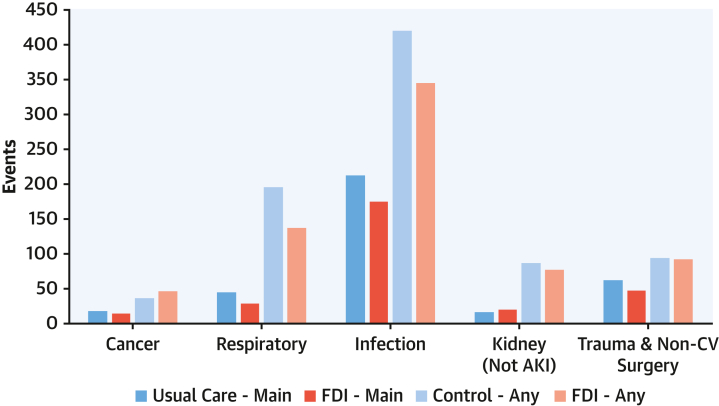
Methods: Patients with heart failure, left ventricular ejection fraction ≤45%, and either transferrin saturation <20% or serum ferritin <100 μg/L were enrolled. Median follow-up was 2.7 years (Q1-Q3: 1.8-3.6 years). A committee adjudicated the main and contributory causes of unplanned hospitalizations and deaths. RRs (rate ratios) for selected recurrent events with 95% CIs are also reported.
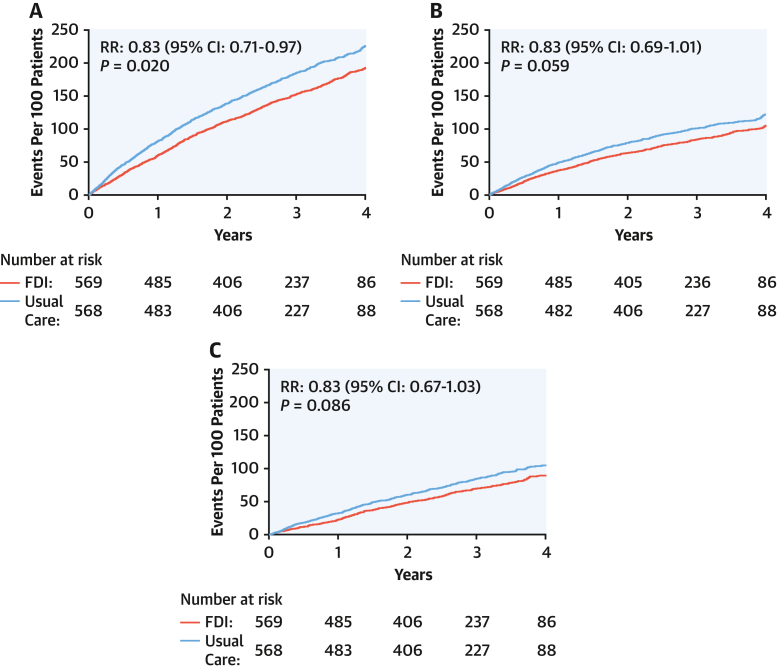
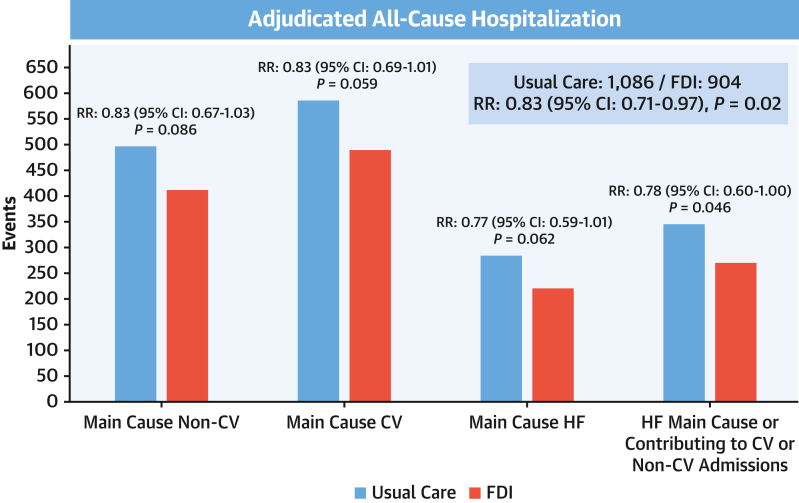
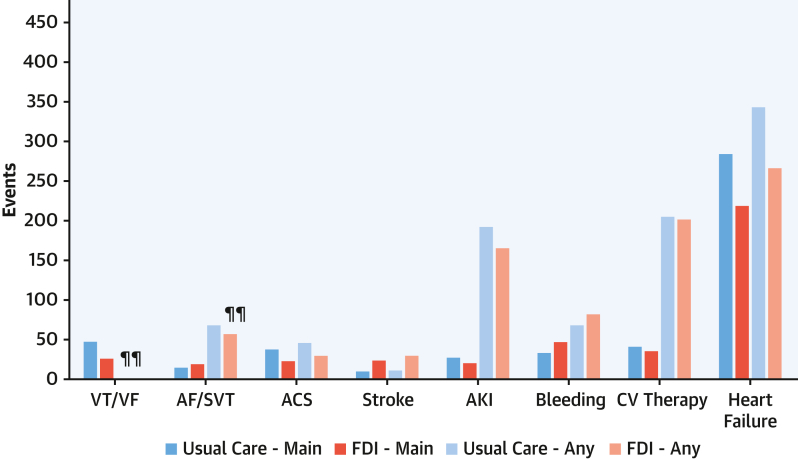
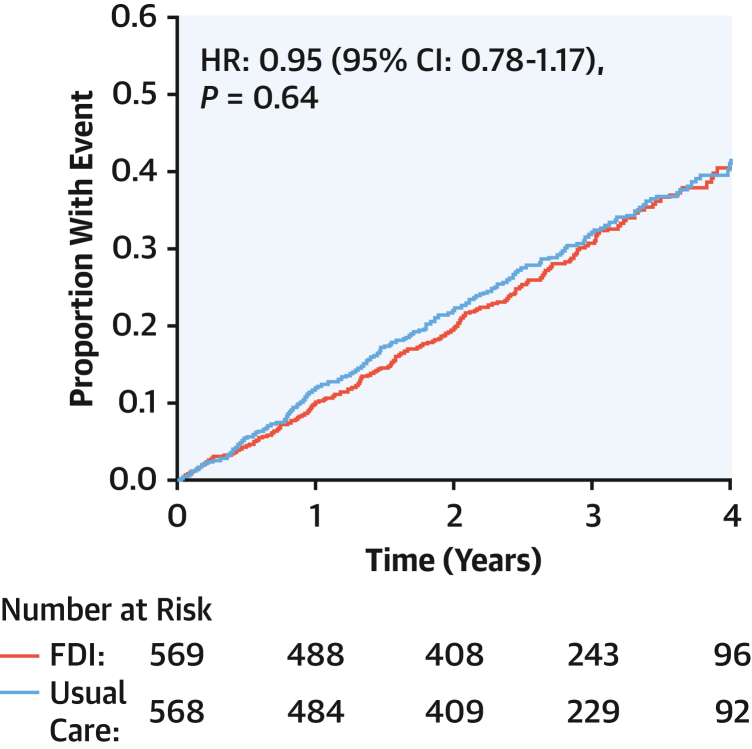
Results: Compared with usual care, patients randomized to FDI had fewer unplanned hospitalizations (RR: 0.83; 95% CI: 0.71-0.97; P = 0.02), with similar reductions in cardiovascular (RR: 0.83; 95% CI: 0.69-1.01) and noncardiovascular (RR: 0.83; 95% CI: 0.67-1.03) hospitalizations, as well as hospitalizations for heart failure (RR: 0.78; 95% CI: 0.60-1.00), respiratory disease (RR: 0.70; 95% CI: 0.53-0.97), or infection (RR: 0.82; 95% CI: 0.66-1.03). Heart failure was the main cause for 26% of hospitalizations and contributed to or complicated a further 12%. Infection caused or contributed to 38% of all hospitalizations, including 27% of heart failure hospitalizations. Patterns of cardiovascular and all-cause mortality were similar for patients assigned to FDI or usual care.
Conclusions: In IRONMAN, FDI exerted similar reductions in cardiovascular and noncardiovascular hospitalizations, suggesting that correcting iron deficiency might increase resistance or resilience to a broad range of problems that cause hospitalizations in patients with heart failure. (Intravenous Iron Treatment in Patients With Heart Failure and Iron Deficiency; NCT02642562).
Keywords: heart failure; hospitalizations; intravenous iron; iron deficiency; randomized trial.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The IRONMAN trial was funded by the British Heart Foundation (grant CS/15/1/31175). Pharmacosmos supplied FDI and gave additional financial support. Dr Cleland has received funding paid to University of Glasgow for other clinical trials and registries from Bristol Myers Squibb and CSL-Vifor; has received consulting fees paid to University of Glasgow from Pharmacosmos, CSL-Vifor, and Biopeutics; has received honoraria for lectures and support for attending meetings paid to University of Glasgow from Pharmacosmos; is chairperson for data monitoring committees for ADAPT-CRT, CMR-Guide, and PROTECT-HF; and has shares or stock options in HeartFelt (noninvasive monitoring) and Viscardia (synchronous diaphragmatic pacing). Dr Pellicori has received consulting fees from Pharmacosmos, Vifor, and Caption Health; has received honoraria for lectures from AstraZeneca; and has received support for attending meetings from Pharmacosmos. Dr Graham has received personal consulting fees from Vifor; and has received personal support for attending meetings from Pharmacosmos. Dr Petrie has received grants/contracts from Boehringer Ingelheim, Roche, SQ Innovations, AstraZeneca, Novartis, Novo Nordisk, Medtronic, Boston Scientific, and Pharmacosmos; has received consulting fees from Akero, Applied Therapeutics, Amgen, AnaCardio, Biosensors, Boehringer Ingelheim, Novartis, AstraZeneca, Novo Nordisk, Abbvie, Bayer, Horizon Therapeutics, Takeda, Cardiorentis, Pharmacosmos, Siemens, Eli Lilly, Vifor, New Amsterdam, Moderna, Teikoku, LIB Therapeutics, and 3R Lifesciences; and has participated on data safety monitoring boards for Moderna and Teikoku. Dr Ahmed has received honoraria for lectures from Pharmacosmos. Dr Squire has received grants/contracts from the British Heart Foundation. Dr Ludman has received honoraria for lectures from AstraZeneca; and is chairperson for the British Cardiovascular Society Guidelines and Practice Committee. Dr Japp has received personal consulting fees from Pharmacosmos; has received honoraria for educational events from Novartis and AstraZeneca; has received support for attending meetings from Novartis; has participated on an advisory board for Pharmacosmos; and is Clinical Lead and Chair for Heart Failure Hub Scotland. Dr Al-Mohammad has received personal honoraria for lectures from AstraZeneca, Janssen, Takeda, and Pharmacosmos; has participated on advisory boards for Novartis, Pharmacosmos, AstraZeneca, Boehringer Ingelheim, and Lilly; is a safety monitoring board member for the REACH-HFpEF Study and a UK-HFpEF registry Executive Steering Committee member; and has received equipment from AstraZeneca. Dr Clark is Chair of the Programme Committee for BCS. Dr Szwejkowski has received support for attending meetings from AstraZeneca. Dr McMurray has received personal consulting fees from Alynylam Pharmaceuticals, Bayer, BMS, Ionis Pharmaceuticals, Novartis, Regeneron Pharmaceuticals, and River 2 Renal Corp; is a director of Global Clinical Trial Partners; has received personal honoraria for lectures from Abbott, Alkem Metabolics, AstraZeneca, Blue Ocean Scientific Solutions Ltd., Boehringer Ingelheim, Canadian Medical and Surgical Knowledge, Emcure Pharmaceuticals, Eris Lifesciences, European Academy of CME, Hikma Pharmaceuticals, Imagica Health, Intas Pharmaceuticals, J.B. Chemicals & Pharmaceuticals, Lupin Pharmaceuticals, Medscape/Heart.Org, ProAdWise Communications, Radcliffe Cardiology, Sun Pharmaceuticals, The Corpus, Translation Research Group, and Translational Medicine Academy; has participated on a data safety monitoring board for George Clinical PTY; and has received funding paid to University of Glasgow for involvement with the following companies/trials: AstraZeneca (DAPA-HF, DELIVER, DETERMINE, DAPA-Resist, DAPA-CKD), Amgen (ATOMIC-HF, COSMIC-HF, GALACTIC-HF), Bayer (FINEARTS), Cardurion (company advisory board), Cytokinetics (GALACTIC-HF), GlaxoSmithKline (ASCEND-D, ASCEND-ND), KBP Biosciences (scientific advisor), and Novartis (PARAGON-HF, PARADISE-MI, PERSPECTIVE, PARACHUTE-HF). Drs Thomson and Robertson have received grants paid to University of Glasgow from the British Heart Foundation and Pharmacosmos. Dr Ford has received grants paid to University of Glasgow from the British Heart Foundation and Pharmacosmos and study drug from Pharmacosmos. Dr Philip Kalra has received funding from Pharmacosmos; has received grants from CSL Vifor, Astellas, Evotec, Pharmacosmos, and Unicyte; has received consulting fees from AstraZeneca, CSL Vifor, Unicyte, and UCB; has received honoraria for lectures from CSL Vifor, AstraZeneca, Pfizer, Pharmacosmos, Napp, and Bayer; and has received support for attending meetings from Pharmacosmos and CSL Vifor. Dr Paul Kalra has received grants paid to University of Glasgow from the British Heart Foundation and Pharmacosmos and to Portsmouth Hospitals University NHS Trust from Pharmacosmos; has received personal consulting fees from Amgen, Boehringer Ingelheim, Pharmacosmos, Servier, and CSL Vifor; has received personal honoraria for lectures from AstraZeneca, Bayer, Novartis, Pfizer, Pharmacosmos, CSL Vifor, and Amgen; has received support for attending meetings from Pharmacosmos; has participated on data safety monitoring boards for the STOP-ACE and EMPRESS-MI trials; and has been Chair-Elect, Chair, and Past Chair for the British Society for Heart Failure. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Desai A.S., Petrie M.C. Centrally adjudicated heart failure outcomes are needed in clinical trials. JACC Heart Fail. 2023;11:418–421. - PubMed
-
- Hicks K.A., Mahaffey K.W., Mehran R., et al. 2017 cardiovascular and stroke endpoint definitions for clinical trials. J Am Coll Cardiol. 2018;71:1021–1034. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
