

Subjective Cognitive Complaints and Anecdotal Descriptions of Postoperative Cognitive Decline: Missing Pieces of the Postoperative Neurocognitive Disorder Puzzle
- PMID: 39443048
- PMCID: PMC11995857
- DOI: 10.1016/j.aan.2024.07.003
Subjective Cognitive Complaints and Anecdotal Descriptions of Postoperative Cognitive Decline: Missing Pieces of the Postoperative Neurocognitive Disorder Puzzle
Abstract
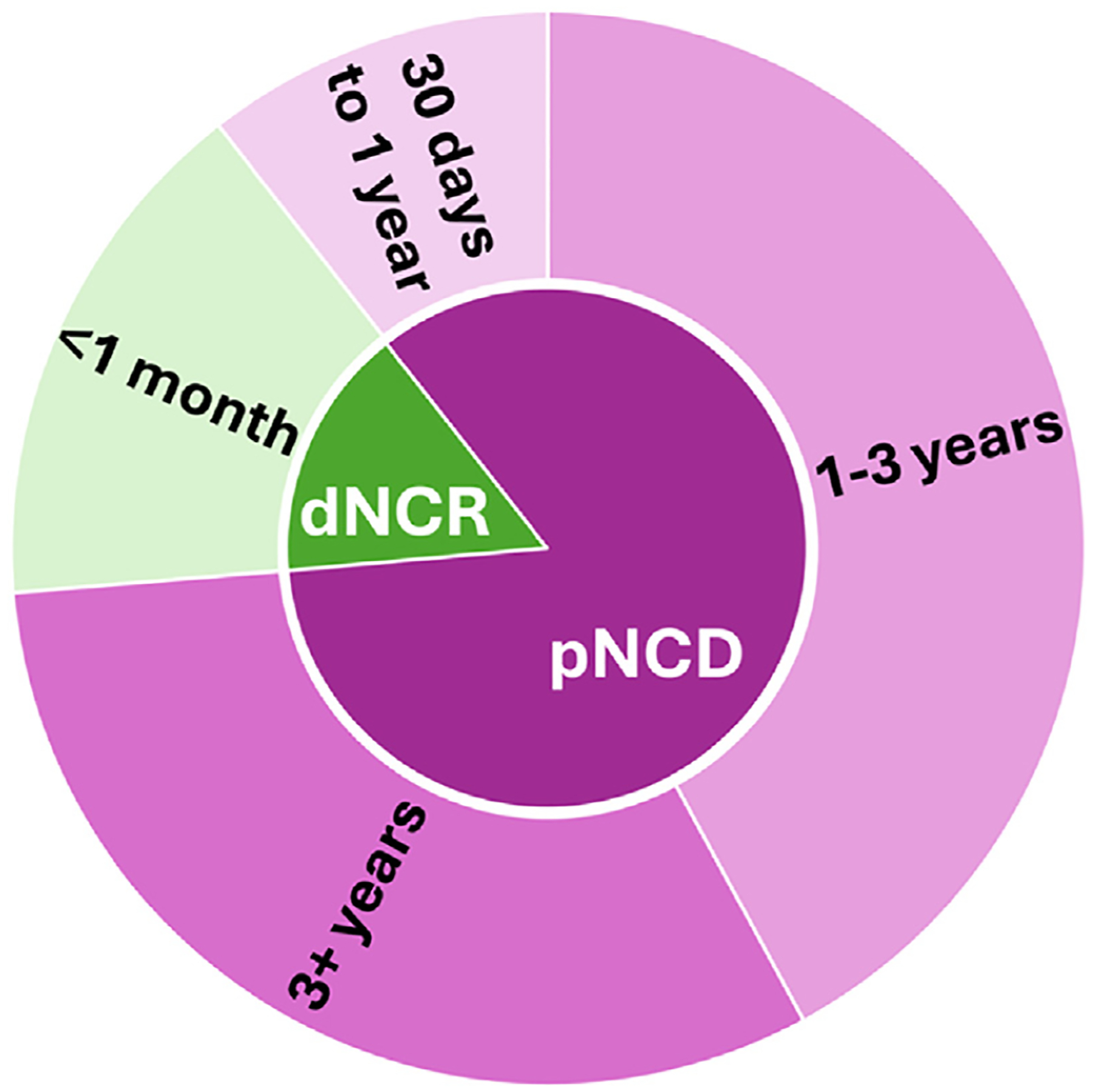
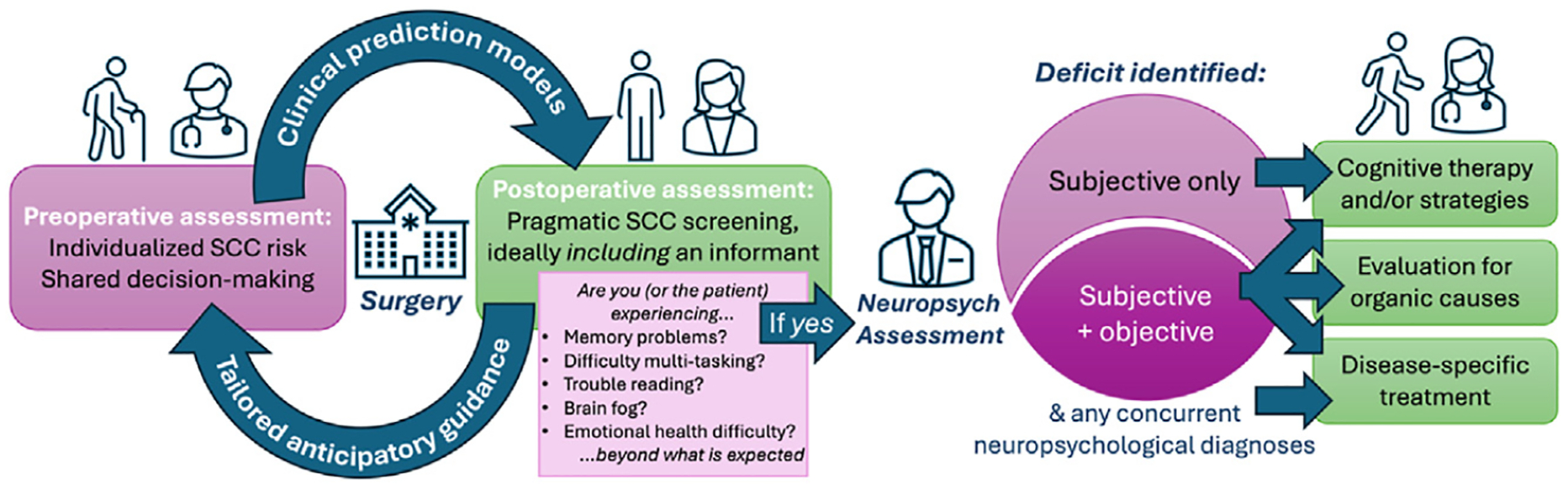
Postoperative cognitive recovery is deeply important to patients and perioperative clinicians. Despite decades of data on "postoperative cognitive decline" (POCD), a research diagnosis based on objective cognitive test performance, perspectives on subjective cognitive complaints (SCC) after modern surgery/anesthesia have not been systematically collected or studied despite their recent inclusion in the 2018 redefinition of "postoperative neurocognitive disorder." The authors describe the alignment between SCC anecdotes and the research diagnosis of POCD, contextualizing these findings using recent literature within and outside anesthesiology. This article prepares anesthesiologists to discuss what is, and is not, known about subjective cognitive recovery after surgery/anesthesia.
Keywords: Postoperative cognitive dysfunction; Postoperative neurocognitive disorder; Subjective cognitive complaints.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure Ms L.Y. Li has no disclosures to report. Dr A.M. Staffaroni reports receiving research support from the National Institute on Aging, United States (NIA) of the National Institutes of Health (NIH), Bluefield Project to Cure FTD, the Alzheimer's Association, United States the Larry L. Hillblom Foundation, United States the Association for Frontotemporal Degeneration, United States the ALS Association, United States and the Rainwater Charitable Foundation, United States; and consulting for Alector Inc, Eli Lilly and Company/Prevail Therapeutics, Passage Bio Inc, and Takeda Pharmaceutical Company; and receiving licensing fees as a coinventor of smartphone cognitive tests. Dr E.L. Whitlock reports receiving research support from the NIA of the NIH.
Figures
Similar articles
-
Effect of Intravenous Lidocaine on Postoperative Cognitive Dysfunction in Patients Undergoing General Anesthesia Surgery: A Systematic Review of a Randomized Controlled Trial.Clin Ther. 2025 Jan;47(1):91-101. doi: 10.1016/j.clinthera.2024.09.027. Epub 2024 Oct 30. Clin Ther. 2025. PMID: 39482176
-
Exploring cognitive function and postoperative neurocognitive recovery after cardiac surgery in older adults (ECPON): a protocol for an observational study.BMJ Open. 2025 Jun 22;15(6):e098208. doi: 10.1136/bmjopen-2024-098208. BMJ Open. 2025. PMID: 40545303 Free PMC article.
-
Intravenous versus inhalational maintenance of anaesthesia for postoperative cognitive outcomes in elderly people undergoing non-cardiac surgery.Cochrane Database Syst Rev. 2018 Aug 21;8(8):CD012317. doi: 10.1002/14651858.CD012317.pub2. Cochrane Database Syst Rev. 2018. PMID: 30129968 Free PMC article.
-
Postoperative Cognitive Decline in Patients Undergoing Major Gynecologic Oncology Surgery: A Pilot Prospective Study.J Obstet Gynaecol Can. 2024 Aug;46(8):102584. doi: 10.1016/j.jogc.2024.102584. Epub 2024 Jun 13. J Obstet Gynaecol Can. 2024. PMID: 38878823
-
Processed electroencephalogram and evoked potential techniques for amelioration of postoperative delirium and cognitive dysfunction following non-cardiac and non-neurosurgical procedures in adults.Cochrane Database Syst Rev. 2018 May 15;5(5):CD011283. doi: 10.1002/14651858.CD011283.pub2. Cochrane Database Syst Rev. 2018. PMID: 29761891 Free PMC article.
References
-
- Romero CS, Urman RD, Luedi MM. Perioperative Evaluation of Brain Health. Anesthesiol Clin 2024;42(1):1–8. - PubMed
-
- Neuro VI. Perioperative covert stroke in patients undergoing non-cardiac surgery (NeuroVISION): a prospective cohort study. Lancet 2019;394(10203):1022–9. - PubMed
-
- Rowley P, Boncyk C, Gaskell A, et al. What do people expect of general anaesthesia? Br J Anaesth 2017;118(4):486–8. - PubMed
-
- Hogan KJ, Bratzke LC, Hogan KL. Informed Consent and Cognitive Dysfunction After Noncardiac Surgery in the Elderly. Anesth Analg 2018;126(2):629–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials