

Real-world Data of Antithrombotic Therapy in Neuroendovascular Therapy: Analysis of JR-NET 4
- PMID: 39443122
- PMCID: PMC11729255
- DOI: 10.2176/jns-nmc.2024-0144
Real-world Data of Antithrombotic Therapy in Neuroendovascular Therapy: Analysis of JR-NET 4
Abstract
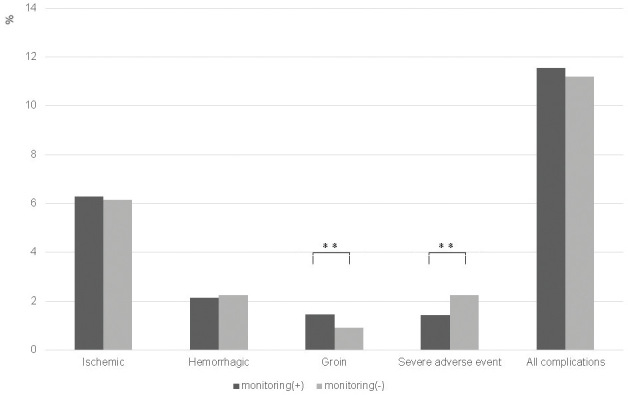
As the number of neuroendovascular therapies in Japan increases, the current trends in periprocedural antithrombotic therapy must be understood.We retrospectively analyzed data on periprocedural antithrombotic therapy in the Japanese Registry of Neuroendovascular Therapy (JR-NET) 4, a nationwide survey carried out in Japan between January 2015 and December 2019. Details on antithrombotic therapy in neuroendovascular therapy for ruptured cerebral aneurysms, unruptured cerebral aneurysms, and percutaneous transluminal angioplasty or stenting were collected from the JR-NET 4 database. These data were analyzed and compared with those from the JR-NET 2 (January 2008 to December 2009) and JR-NET 3 (January 2010 to December 2014). A total of 36,560 cases were analyzed in the JR-NET 4. The frequency of preprocedural dual antiplatelet therapy (DAPT) significantly increased from the JR-NET 2 to 4 (48.1%, 53.4%, and 62.3%, respectively; P < 0.001), whereas the frequency of monotherapy significantly decreased (15.7%, 13.9%, and 8%, respectively; P < 0.001). Postprocedural antiplatelet therapy exhibited similar trends, and postprocedural anticoagulant therapy was discontinued. Particularly, heparin use significantly decreased from the JR-NET 2 to 4 (23.4% vs. 12.7% vs. 7.9%, respectively; P < 0.001). In terms of periprocedural complications, the incidence of ischemic complications increased from the JR-NET 3 to 4 (5.8% vs. 6.2%; P = 0.05). In the JR-NET 4, severe adverse events and hemorrhagic and all complications were significantly more frequent in the preprocedural triple or more therapy group.The rate of postprocedural anticoagulant therapy decreased, whereas that of antiplatelet therapy increased. Overall, in Japan, periprocedural DAPT has become increasingly common.
Keywords: anticoagulant therapy; antiplatelet therapy; dual antiplatelet therapy; neuroendovascular therapy.
Conflict of interest statement
All authors who are members and non-members of the Japan Neurosurgical Society (JNS) have registered self-reported COI disclosure statements through the website for JNS. Dr. Nobuyuki Sakai reports a research grant from Japan Lifeline, Kaneka, Medtronic, Terumo, and TG Medical; lecturer's fees from Asahi-Intecc, Kaneka, Medtronic, Stryker, and Terumo; membership on the advisory boards for Johnson & Johnson, Medtronic, and Terumo outside the submitted work. Dr. Yamagami Hiroshi discloses research grants from Bristol Myers Squibb; lecturer's fees from Stryker, Medtronic, Johnson & Johnson, Medico's Hirata, Daiichi Sankyo, Bayer, and Otsuka Pharmaceutical; and membership of the advisory boards for Daiichi Sankyo. Dr. Imamura Hirotoshi discloses lecturer's fees from Medtronic, Terumo, Daiichi Sankyo, Stryker, Johnson & Johnson, and Asahi-Intecc. Dr. Yukiko Enomoto received research grants from Sysmex and Medtronic, and a lecturer's fee from Daiichi Sankyo, Otsuka Pharmaceutical Co. Ltd, Stryker, and Medtronic. Dr. Tetsu Satow reports a research grant from CANON Medical Systems, a lecturer's fee from Medtronic, and a consulting fee from Kaneka Medix, outside the submitted work. Other co-authors have no conflict of interest for this manuscript.
Figures


References
-
- Delgado Almandoz JE, Crandall BM, Scholz JM, et al. : Pre-procedure P2Y12 reaction units value predicts perioperative thromboembolic and hemorrhagic complications in patients with cerebral aneurysms treated with the Pipeline Embolization Device. J Neurointerv Surg 5: iii3-ii10, 2013 - PubMed
-
- McKevitt FM, Randall MS, Cleveland TJ, Gaines PA, Tan KT, Venables GS: The benefits of combined anti-platelet treatment in carotid artery stenting. Eur J Vasc Endovasc Surg 29: 522-527, 2005 - PubMed
-
- Bates ER, Babb JD, Casey DE, et al. : ACCF/SCAI/SVMB/SIR/ASITN 2007 Clinical Expert Consensus Document on carotid stenting. Vasc Med 12: 35-83, 2007 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials