Methodologies and clinical applications of lower limb muscle ultrasound in critically ill patients: a systematic review and meta-analysis
- PMID: 39443352
- PMCID: PMC11499498
- DOI: 10.1186/s13613-024-01395-y
Methodologies and clinical applications of lower limb muscle ultrasound in critically ill patients: a systematic review and meta-analysis
Abstract
Background: Reduced muscle mass upon admission and development of muscle wasting are frequent in critically ill patients, and linked to unfavorable outcomes. Muscle ultrasound is a promising instrument for evaluating muscle mass. We summarized the findings of lower limb muscle ultrasound values and investigated how the muscle ultrasound parameters of the examination or the patient characteristics influence the results.
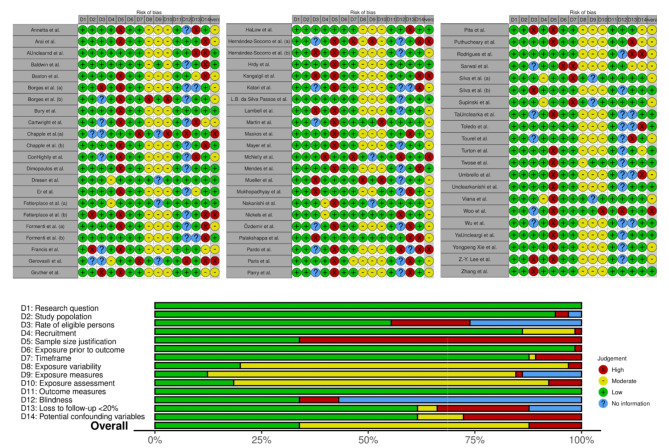
Methods: Systematic review and meta-analysis of studies of lower limb ultrasound critically ill adults. PubMed, CINAHL, Embase, PEDro and Web of Science were searched. PRISMA guidelines were followed, and studies evaluated with the appropriate NIH quality assessment tool. A meta-analysis was conducted to compare the values at admission, short and long follow-up during ICU stay, and the association between baseline values and patient characteristics or ultrasound parameters was investigated with a meta-regression.
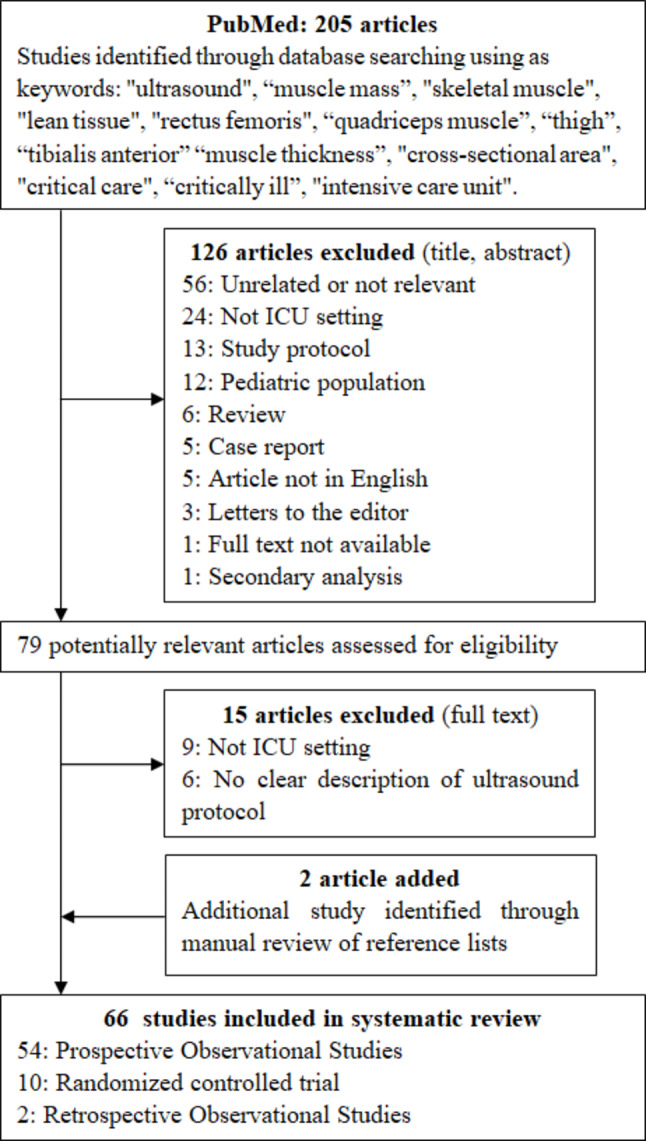
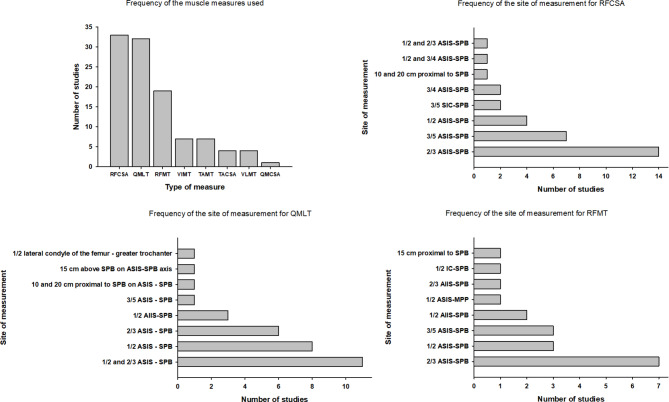
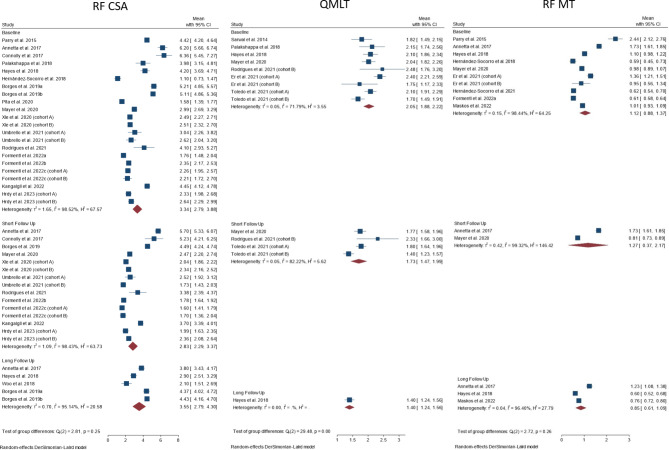
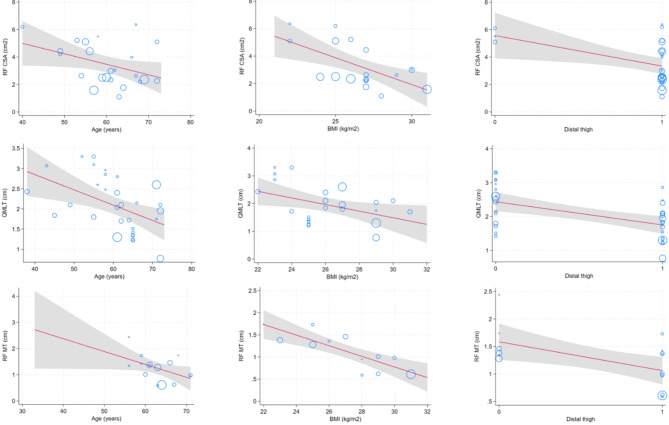
Results: Sixty-six studies (3839 patients) were included. The main muscles investigated were rectus femoris cross-sectional area (RF-CSA, n = 33/66), quadriceps muscle layer thickness (n = 32/66), and rectus femoris thickness (n = 19/66). Significant differences were found in the anatomical landmark and ultrasound settings. At ICU admission, RF-CSA ranged from 1.1 [0.73-1.47] to 6.36 [5.45-7.27] cm2 (pooled average 2.83 [2.29-3.37] cm2) with high heterogeneity among studies (I2 = 98.43%). Higher age, higher BMI, more distal landmark and the use of probe compression were associated with lower baseline muscle mass.
Conclusions: Measurements of muscle mass using ultrasound varied with reference to patient characteristics, patient position, anatomical landmarks used for measurement, and the level of compression applied by the probe; this constrains the external validity of the results and highlights the need for standardization.
Study registration: PROSPERO CRD42023420376.
Keywords: Critically ill; Lean body mass; Meta-analysis; Muscle ultrasound; Muscle wasting; Systematic review; Ultrasound.
© 2024. The Author(s).
Conflict of interest statement
MU has received speaker fees from Baxter, Fresenius Kabi and Nestlè. The other authors declare that they have no conflicts of interest.
Figures