

Evaluation of clinical and radiographic warning signs for prediction of oroantral communication following tooth extractions
- PMID: 39443353
- PMCID: PMC11499406
- DOI: 10.1007/s00784-024-06000-x
Evaluation of clinical and radiographic warning signs for prediction of oroantral communication following tooth extractions
Abstract
Objectives: Oroantral communication (OAC) is a relatively common and mild complication of maxillary tooth extractions. Preoperative prediction of OAC can reduce treatment duration and prepare both operators and patients for the procedure. This study aims to identify alarming radiographic and clinical indicators that can predict OAC therefore assisting clinical decision making to practicing general dentists.
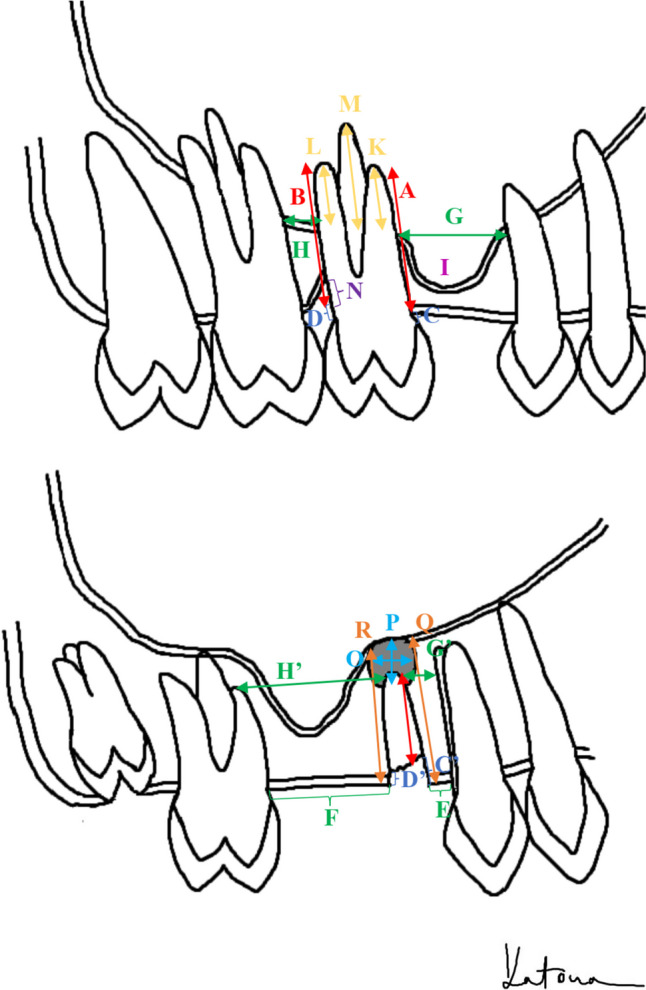
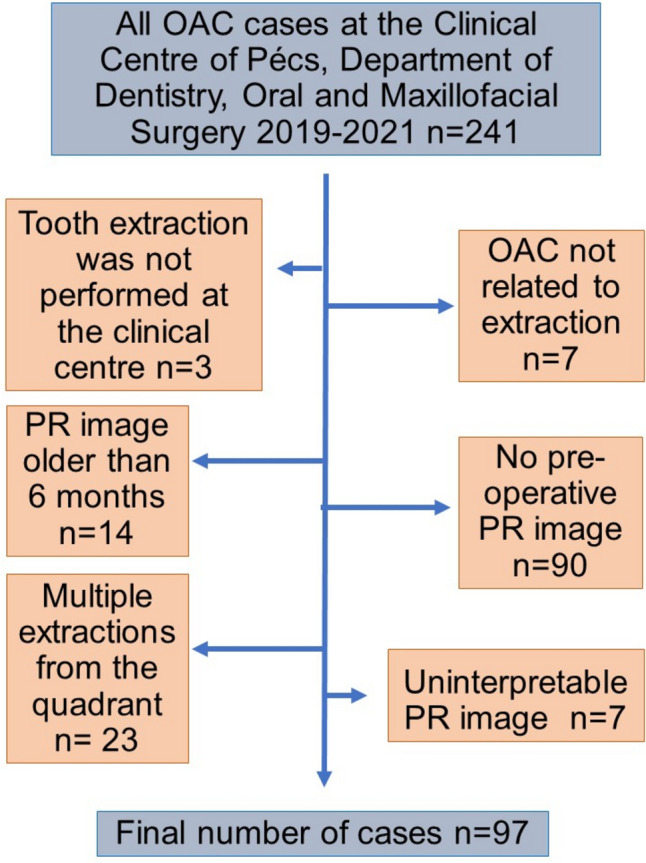
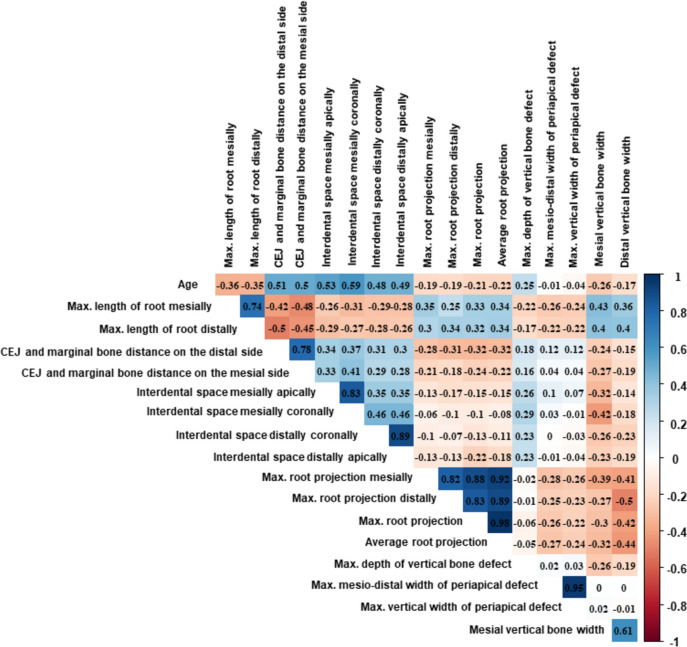
Methods: In this retrospective case-control study the OAC group consisting of 97 cases and a control group twice the size was established. Clinical data were collected, and measurements were conducted separately by two blinded observers on digital panoramic radiographs. Inter-rater reliability was assessed. In case of disagreement a third observer's results were utilized. The correlation between OAC and demographic data (age, sex), as well as various factors assessed on panoramic radiographs (including, but not limited to, the length of the root, root projection into the sinus, bone width, presence of mesial and distal adjacent teeth), was statistically evaluated.
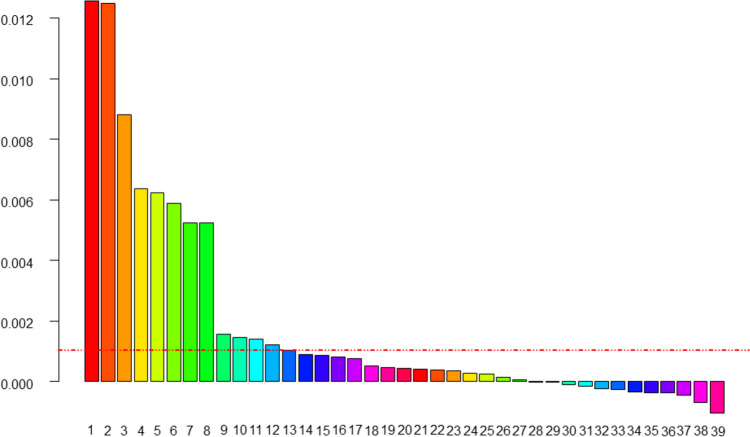
Results: Inter-rater reliability was found to be excellent. Several factors were identified as potential predictors of OAC. According to our model, the strongest predictors were the distance between the cemento-enamel junction and marginal bone, extent of root projection into the sinus, presence of sinus recess around the roots, angulation, and absence of the mesial adjacent tooth.
Conclusions: Well-defined measurements on panoramic radiographs may aid in predicting OAC. Further prospective investigations are necessary to confirm these indicators and address factors related to clinical examination and operation.
Clinical relevance: We present several clinical and radiographic warning signs of OAC that can facilitate pre-extraction decision-making.
Keywords: Intraoperative Complications; Maxillary Sinus; Oroantral Fistula; Orthopantomography; Panoramic radiograph; Tooth Extraction.
© 2024. The Author(s).
Conflict of interest statement
We report no competing interests.
Figures

References
-
- Punwutikorn J, Waikakul A, Pairuchvej V (1994) Clinically significant oroantral communications - a study of incidence and site. Int J Oral Maxillofac Surg 23:19–21. 10.1016/S0901-5027(05)80320-0 - PubMed
-
- Miclotte I, Agbaje JO, Spaey Y et al (2018) Incidence and treatment of complications in patients who had third molars or other teeth extracted. Br J Oral Maxillofac Surg 56:388–393. 10.1016/j.bjoms.2018.02.001 - PubMed
-
- Kiencało A, Jamka-Kasprzyk M, Panaś M, Wyszyńska-Pawelec G (2021) Analysis of complications after the removal of 339 third molars. Dent Med Probl 58:75–60. 10.17219/dmp/127028 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
