

Clinical usefulness of digital twin guided virtual amiodarone test in patients with atrial fibrillation ablation
- PMID: 39443659
- PMCID: PMC11499921
- DOI: 10.1038/s41746-024-01298-z
Clinical usefulness of digital twin guided virtual amiodarone test in patients with atrial fibrillation ablation
Abstract
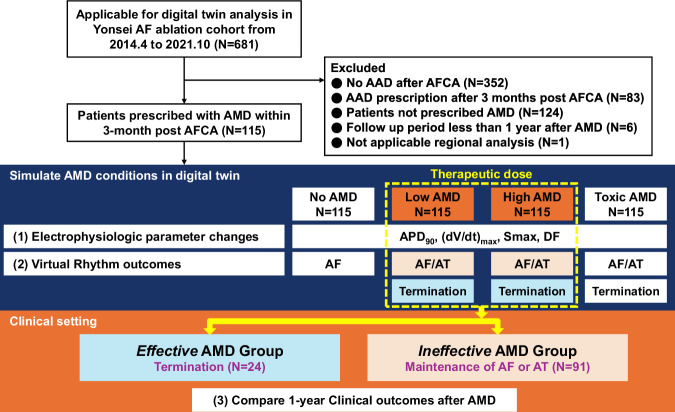
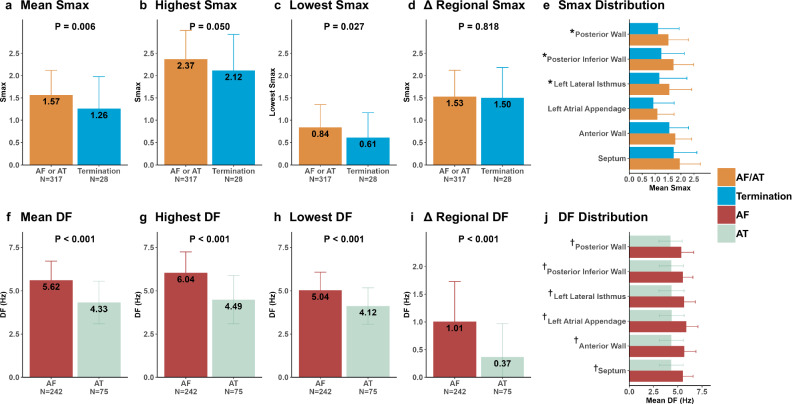
It would be clinically valuable if the efficacy of antiarrhythmic drugs could be simulated in advance. We developed a digital twin to predict amiodarone efficacy in high-risk atrial fibrillation (AF) patients post-ablation. Virtual left atrium models were created from computed tomography and electroanatomical maps to simulate AF and evaluate its response to varying amiodarone concentrations. As the amiodarone concentration increased in the virtual setting, action potential duration lengthened, peak upstroke velocities decreased, and virtual AF termination became more frequent. Patients were classified into effective (those with virtually terminated AF at therapeutic doses) and ineffective groups. The one-year clinical outcomes after AF ablation showed significantly better results in the effective group compared to the ineffective group, with AF recurrence rates of 20.8% vs. 45.1% (log-rank p = 0.031, adjusted hazard ratio, 0.37 [0.14-0.98]; p = 0.046). This study highlights the potential of a digital twin-guided approach in predicting amiodarone's effectiveness and improving personalized AF management. Clinical Trial Registration Name: The Evaluation for Prognostic Factors After Catheter Ablation of Atrial Fibrillation: Cohort Study, Registration number: NCT02138695. The date of registration: 2014-05. URL: https://www.clinicaltrials.gov ; Unique identifier: NCT02138695.
© 2024. The Author(s).
Conflict of interest statement
H.P. and B.L. are the inventors of a patent application (Patent Number: 10-2257498) for the CUVIA system, a patented technology that we utilized to create digital twin in our study. H.P. and O.K. are the inventors of CUVIA-AAD and are currently preparing a patent, including a collaboration with Waycen Corporation for CUVIA-AAD, an automated analysis system for antiarrhythmic drugs. Other authors have no relevant financial or non-financial interests to disclose.
Figures



References
-
- Hindricks, G. et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J.42, 373–498 (2021). - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
