

Association between preoperative shock index and hypotension after spinal anesthesia for non-elective cesarean section: a prospective cohort study
- PMID: 39443886
- PMCID: PMC11515677
- DOI: 10.1186/s12871-024-02766-5
Association between preoperative shock index and hypotension after spinal anesthesia for non-elective cesarean section: a prospective cohort study
Abstract
Background: Shock index (SI) is calculated as heart rate divided by systolic blood pressure. In the obstetric population, SI of ≥ 0.9 is associated with maternal adverse outcomes. Our primary aim was to investigate the association between SI and post-spinal hypotension in non-elective cesarean section.
Methods: In this prospective, observational study, term parturient of ASA physical status II, and urgency categories 2 and 3, undergoing non-elective cesarean section with spinal anesthesia were enrolled. We performed univariable and multivariable logistic regression to explore the association between baseline SI (categorized as < 0.9 and ≥ 0.9) and hypotension after spinal anesthesia. The diagnostic ability of the baseline SI to predict post-spinal hypotension was assessed using ROC (receiver operating characteristics) curves.
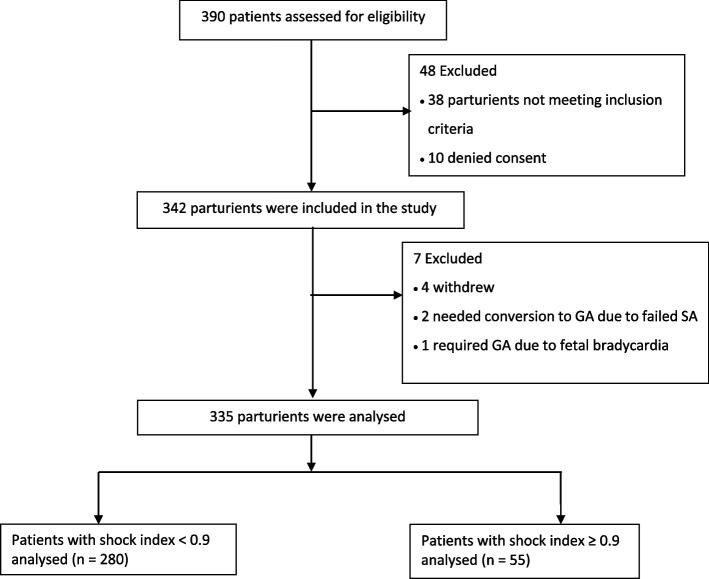
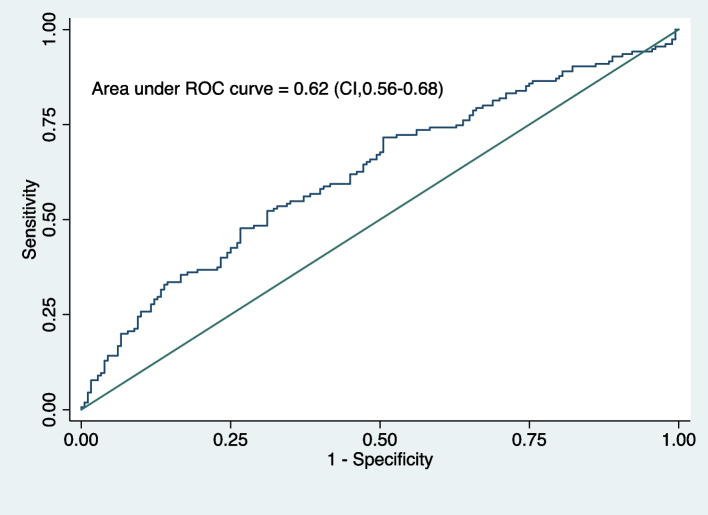
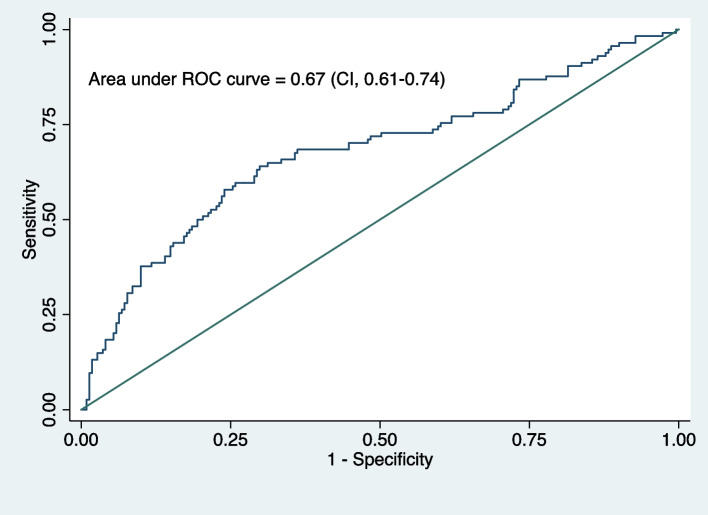
Results: Three hundred forty-two parturient were recruited, and among them, 335 were analyzed. One hundred fifty-five (46.27%) parturients developed post-spinal hypotension, and 114 (34.03%) reported post-delivery hypotension. Preoperative SI (adjusted odds ratio [AOR], 2.77; 95% CI, 1.15-6.66; p = 0.023) and thoracic sensory block height > 4 (AOR, 2.33; 95%CI, 1.14-4.76; p = 0.020) were associated with post-spinal hypotension. Preoperative SI (AOR, 4.34; 95%CI, 1.72-10.94; p = 0.002) and anxiety (AOR,1.22; 95%CI, 1.06-1.40; p = 0.004) were associated with post-delivery hypotension. Area under the ROC curve for SI alone in predicting hypotension before and after delivery was 0.53 (95%CI 0.49-0.57) and 0.56 (95%CI 0.51-0.60) respectively. However, the model performance as reflected by ROC curve for the multivariable logistic regression analysis was 0.623 for post-spinal hypotension and 0.679 for post-delivery hypotension, respectively.
Conclusion: In parturients undergoing non-elective cesarean section, baseline SI ≥ 0.9 was associated with post-spinal and post-delivery hypotension. While the SI alone showed limited predictive power for post-spinal and post-delivery hypotension, integrating it with other risk factors improved the model's predictive ability.
Trial registration: Registration number: NCT04692870. Date of registration: 05/01/2021. Website: https://clinicaltrials.gov .
Keywords: Cesarean section; Hypotension; Shock Index; Spinal Anesthesia.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Role of pleth variability index for predicting hypotension after spinal anesthesia for cesarean section.Int J Obstet Anesth. 2014 Nov;23(4):324-9. doi: 10.1016/j.ijoa.2014.05.011. Epub 2014 Jun 10. Int J Obstet Anesth. 2014. PMID: 25262278
-
Transient Tachypnea of Newborns Is Associated With Maternal Spinal Hypotension During Elective Cesarean Delivery: A Retrospective Cohort Study.Anesth Analg. 2019 Jul;129(1):162-167. doi: 10.1213/ANE.0000000000004064. Anesth Analg. 2019. PMID: 30768454
-
Differential Roles of the Right and Left Toe Perfusion Index in Predicting the Incidence of Postspinal Hypotension During Cesarean Delivery.Anesth Analg. 2017 Nov;125(5):1560-1566. doi: 10.1213/ANE.0000000000002393. Anesth Analg. 2017. PMID: 28795968
-
Effects of neuraxial anesthesia in sitting and lateral positions on maternal hemodynamics in cesarean section: A systematic review and meta-analysis.PLoS One. 2024 May 17;19(5):e0303256. doi: 10.1371/journal.pone.0303256. eCollection 2024. PLoS One. 2024. PMID: 38758837 Free PMC article.
-
Evidence-Based Prevention Strategies for the Management of Spinal Anesthesia-Induced Hypotension in Healthy Parturients Undergoing Elective Cesarean Delivery.AANA J. 2022 Aug;90(4):311-316. AANA J. 2022. PMID: 35943759
References
-
- Reynolds F, Seed PT. Anaesthesia for Caesarean section and neonatal acid-base status: a meta-analysis. Anaesthesia. 2005;60:636–53. - PubMed
-
- Mavridou I, Stewart A, Fernando R. Maternal hypotension during spinal anesthesia for cesarean delivery. Curr Anesthesiol Rep. 2013;3:282–91.
-
- Mohta M, Aggarwal M, Sethi AK, Harisinghani P, Guleria K. Randomized double-blind comparison of ephedrine and phenylephrine for management of post-spinal hypotension in potential fetal compromise. Int J Obstet Anesth. 2016;27:32–40. - PubMed
-
- Ngan Kee WD, Khaw KS, Lau TK, Ng FF, Chui K, Ng KL. Randomised double-blinded comparison of phenylephrine vs ephedrine for maintaining blood pressure during spinal anaesthesia for non-elective Caesarean section. Anaesthesia. 2008;63:1319–26. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
