

Effects of atrial fibrillation ablation on arrhythmia burden and ventricular function in end-stage heart failure: Lessons from CASTLE-HTx
- PMID: 39444312
- PMCID: PMC11860721
- DOI: 10.1002/ejhf.3505
Effects of atrial fibrillation ablation on arrhythmia burden and ventricular function in end-stage heart failure: Lessons from CASTLE-HTx
Abstract
Aims: The CASTLE-HTx trial showed the benefit of atrial fibrillation (AF) ablation compared to medical therapy in decreasing mortality, need for left ventricular assist device implantation or heart transplantation (HTx) in patients with end-stage heart failure (HF). Herein we describe the effects of catheter ablation on AF burden, arrhythmia recurrences, and ventricular function in end-stage HF.
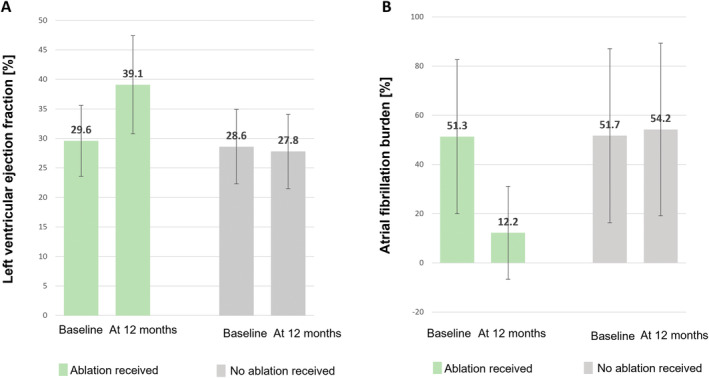
Methods and results: The CASTLE-HTx protocol randomized 194 patients in end-stage HF with AF to catheter ablation and medical therapy or medical therapy alone. AF burden, left ventricular ejection fraction (LVEF), and type of AF were assessed at baseline and at each follow-up visit. Overall, 97 patients received ablation; 66 patients (68%) underwent pulmonary vein isolation (PVI) and 31 patients (32%) were treated with PVI and additional ablation. Electroanatomic mapping showed the extent of left atrial low voltage (cardiomyopathy) >10% in 31 (31.9%) patients. At 12 months post-ablation, persistent AF was present in 31/89 patients (34.8%), which was significantly less frequent compared to baseline (p = 0.0001). Median AF burden reduction was 36.3 (interquartile range 13.6-63.3) percentage points at 12 months and LVEF improved from 29.2 ± 6.2% to 39.1 ± 8.3% (p < 0.001) following ablation. AF burden reduction <50% was significantly associated with LVEF improvement ≥5% at 12 months after ablation (p = 0.017).
Conclusion: Atrial fibrillation ablation in end-stage HF leads to a substantial decrease in AF burden, a regression from persistent to paroxysmal AF and notably improved LVEF. Favourable ablation outcomes were observed in patients regardless of the presence or absence of signs indicating left atrial cardiomyopathy.
Keywords: Atrial fibrillation; Catheter ablation; Heart failure; Heart transplantation; Left ventricular assist device.
© 2024 The Author(s). European Journal of Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Figures

Similar articles
-
Prognostic impact of diagnosis-to-ablation time on outcomes following catheter ablation in persistent atrial fibrillation and left ventricular systolic dysfunction.Heart Rhythm. 2025 Jun;22(6):1429-1436. doi: 10.1016/j.hrthm.2024.09.059. Epub 2024 Sep 27. Heart Rhythm. 2025. PMID: 39343117 Clinical Trial.
-
Different Approaches to Atrial Fibrillation Ablation in Heart Failure Patients: Temporal Trends and Clinical Outcomes.JACC Clin Electrophysiol. 2025 May;11(5):942-952. doi: 10.1016/j.jacep.2024.12.004. Epub 2025 Jan 29. JACC Clin Electrophysiol. 2025. PMID: 39895449
-
Effects of Atrial Fibrillation Ablation for Heart Failure With Preserved Ejection Fraction: Insights From CABANA.JACC Heart Fail. 2025 May;13(5):785-794. doi: 10.1016/j.jchf.2025.01.029. Epub 2025 Apr 16. JACC Heart Fail. 2025. PMID: 40243977 Clinical Trial.
-
Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evaluation.Health Technol Assess. 2008 Nov;12(34):iii-iv, xi-xiii, 1-198. doi: 10.3310/hta12340. Health Technol Assess. 2008. PMID: 19036232
-
Catheter ablation for atrial fibrillation in patients with left ventricular systolic dysfunction. A systematic review and meta-analysis.J Card Fail. 2011 Nov;17(11):964-70. doi: 10.1016/j.cardfail.2011.07.009. Epub 2011 Sep 9. J Card Fail. 2011. PMID: 22041335
Cited by
-
Computational modelling of the pro- and antiarrhythmic effects of atrial high rate-dependent trafficking of small-conductance calcium-activated potassium channels.J Physiol. 2025 Jul 20:10.1113/JP288659. doi: 10.1113/JP288659. Online ahead of print. J Physiol. 2025. PMID: 40685564 Free PMC article.
References
-
- Santhanakrishnan R, Wang N, Larson MG, Magnani JW, McManus DD, Lubitz SA, et al. Atrial fibrillation begets heart failure and vice versa: Temporal associations and differences in preserved versus reduced ejection fraction. Circulation 2016;133:484–492. 10.1161/CIRCULATIONAHA.115.018614 - DOI - PMC - PubMed
-
- Di Biase L, Mohanty P, Mohanty S, Santangeli P, Trivedi C, Lakkireddy D, et al. Ablation versus amiodarone for treatment of persistent atrial fibrillation in patients with congestive heart failure and an implanted device: Results from the AATAC multicenter randomized trial. Circulation 2016;133:1637–1644. 10.1161/CIRCULATIONAHA.115.019406 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
