

Spontaneous Autoamputation of Adnexa
- PMID: 39444420
- PMCID: PMC11495857
- DOI: 10.4293/CRSLS.2024.00025
Spontaneous Autoamputation of Adnexa
Abstract
Introduction: Acquired ovarian torsion is an uncommon gynecologic emergency that afflicts women of reproductive age and requires correction by surgery. A rare complication of asymptomatic ovarian torsion can be necrosis and autoamputation of the adnexal structures.
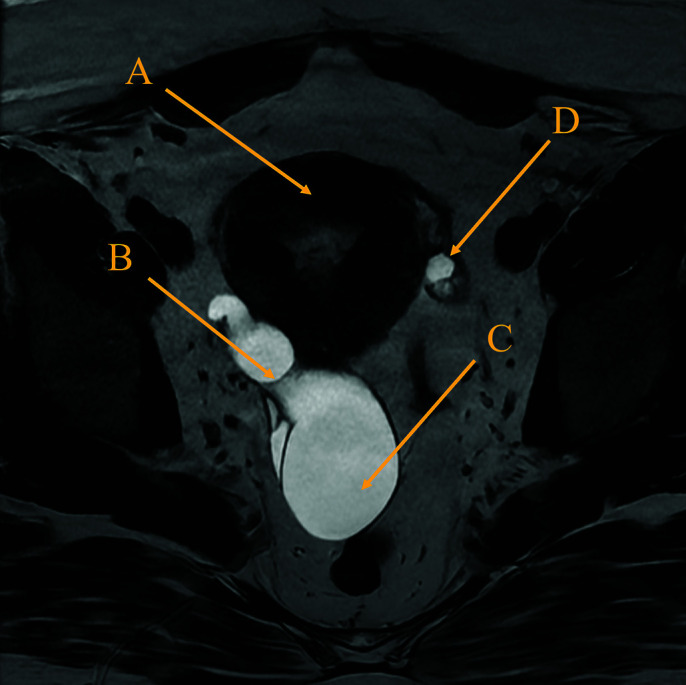
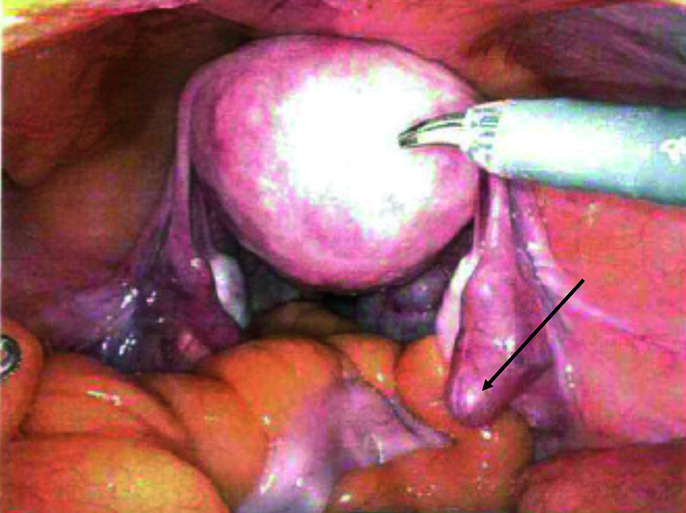
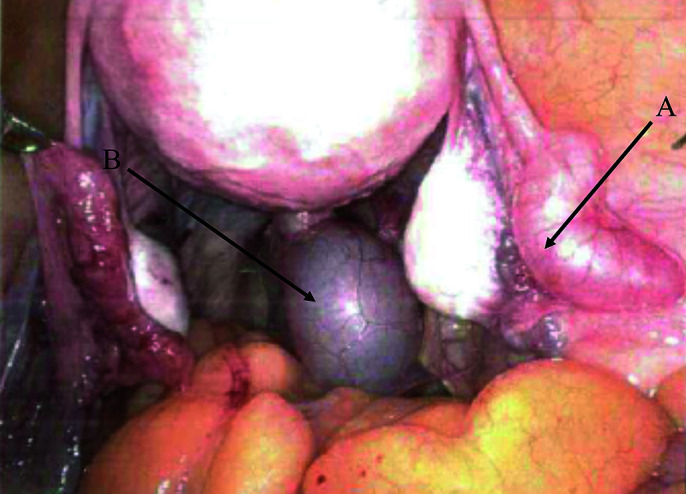
Case description: A 28-year-old nulliparous woman presented with irregular menses since puberty associated with dysmenorrhea, menorrhagia, and nausea, and that did not improve with trials of oral hormone therapy. Ultrasound and pelvic MRI revealed a large, tubular-cystic mass separated from the right ovary and tubo-ovarian junction. Intraoperative findings revealed filmy adhesions and fimbriae emanating from this cystic lesion, as well as dilation of the medial portion of the right fallopian tube. Histopathology reported dilated, cystic structures with focal tubal-type epithelial lining, and a dilated fallopian tube lumen, consistent with hydrosalpinx.
Discussion: Autoamputation of fallopian tube is a rare but serious complication of adnexal torsion that should be treated promptly via intraoperative detorsion.
Keywords: Adnexal torsion; Autoamputation; Ovarian torsion.
© 2024 by SLS, Society of Laparoscopic & Robotic Surgeons.
Conflict of interest statement
Conflict of interests: none.
Figures
Similar articles
-
Isolated torsion of the fallopian tube in a menopausal woman and a pre-pubertal girl: two case reports.J Med Case Rep. 2015 Nov 17;9:258. doi: 10.1186/s13256-015-0745-y. J Med Case Rep. 2015. PMID: 26572791 Free PMC article.
-
Hydrosalpinx with adnexal torsion in an adolescent virgin patient--A diagnostic dilemma: case report and review of the literature.J Pediatr Adolesc Gynecol. 2006 Aug;19(4):297-9. doi: 10.1016/j.jpag.2006.05.016. J Pediatr Adolesc Gynecol. 2006. PMID: 16873035 Review.
-
Fallopian tube torsion in the pediatric age group: radiologic evaluation.J Ultrasound Med. 2014 Sep;33(9):1697-704. doi: 10.7863/ultra.33.9.1697. J Ultrasound Med. 2014. PMID: 25154955
-
The "Double Ovary" Sign: A Unique Sonographic Observation in Isolated Fallopian Tube Torsion.J Ultrasound Med. 2023 Aug;42(8):1881-1886. doi: 10.1002/jum.16208. Epub 2023 Mar 7. J Ultrasound Med. 2023. PMID: 36880675
-
Isolated torsion of the fallopian tube: a case report and review of the literature.Clin Exp Obstet Gynecol. 2004;31(3):235-8. Clin Exp Obstet Gynecol. 2004. PMID: 15491073 Review.
References
-
- Beyth Y, Bar-On E. Tuboovarian autoamputation and infertility. Fertil Steril. 1984;42(6):932–934. - PubMed
-
- Sankaran S, Shahid A, Odejinmi F. Autoamputation of the fallopian tube after chronic adnexal torsion. J Minim Invasive Gynecol. 2009;16(2):219–221. - PubMed
-
- Focseneanu MA, Omurtag K, Ratts VS, Merritt DF. The auto-amputated adnexa: a review of findings in a pediatric population. J Pediatr Adolesc Gynecol. 2013;26(6):305–313. - PubMed
-
- Sasaki KJ, Miller CE. Adnexal torsion: review of the literature. J Minim Invasive Gynecol. 2014;21(2):196–202. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources