

Indocyanine green fluorescence imaging: Assessment of perfusion at pancreatic resection margin during pancreatoduodenectomy: A cross sectional study
- PMID: 39444730
- PMCID: PMC11497489
- DOI: 10.1002/hsr2.70153
Indocyanine green fluorescence imaging: Assessment of perfusion at pancreatic resection margin during pancreatoduodenectomy: A cross sectional study
Abstract
Background: Clinically relevant-postoperative pancreatic fistula (CR-POPF) is one of the dreaded complications of pancreatoduodenectomy. Vascularity of the stump of the pancreas during pancreatico-enteric anastomosis is considered one of the major determinants of POPF. Indocyanine green (ICG) is one of the modality for vascular assessment; hence, we aimed to evaluate the role of ICG fluorescence imaging to assess the vascularity of the pancreatic stump during pancreatoduodenectomy.
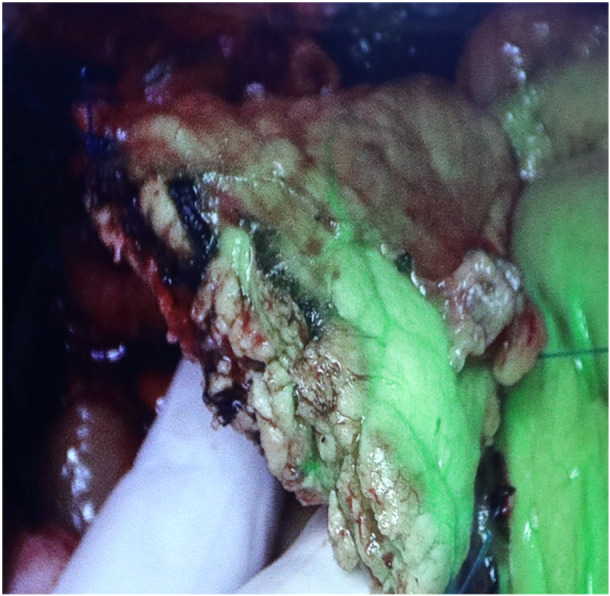
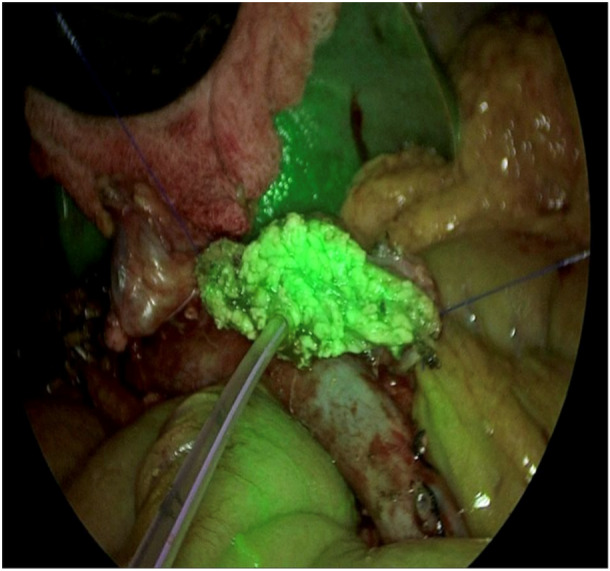
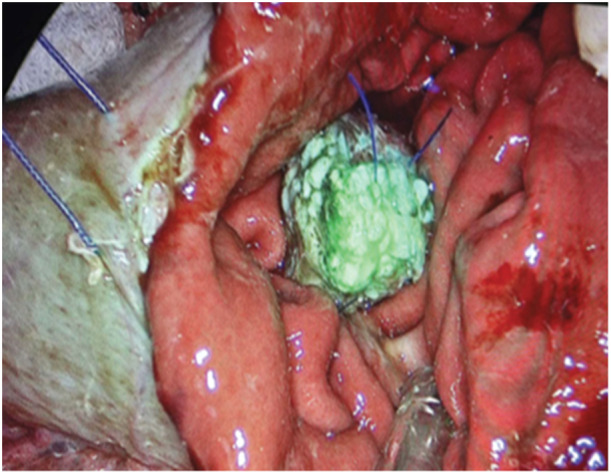
Methodology: The study was conducted at Kathmandu Medical College, Kathmandu, Nepal, during the period of 1 year (June 01, 2022-July 31, 2023). All of the patients who were undergoing pancreatoduodenectomy were included in the study. In all cases, intraoperatively, ICG fluorescence detection at the pancreatic stump margin was evaluated using near-infrared light.
Results: A total of 28 patients underwent PD during this period. The ICG fluorescence imaging was positive at the pancreatic stump margin in 25 out of the 28 patients (89%), and in three cases, the florescence was negative. In patients who had negative fluorescence, revision of the stump margin was performed. Clinically relevant POPF was noted in 2 out of 28 cases, which had a soft pancreas with a small duct, although the pancreatic stump margin had good ICG florescence per-operatively.
Conclusion: ICG is inexpensive and a safe dye to use in clinical practice. We can objectively assess the pancreatic stump vascularity using intraoperative ICG fluorescence imaging, thereby potentially decreasing postoperative pancreatic fistula.
Keywords: fluorescence; indocyanine green; pancreatic stump; pancreatoduodenectomy; perfusion.
© 2024 The Author(s). Health Science Reports published by Wiley Periodicals LLC.
Conflict of interest statement
The authors do not have any conflicts of interest to disclose. This study was presented at the 34th World Congress of the International Association of Surgeons, Gastroenterologists, and Oncologists (IASGO) in Verona, Italy, in September 2023.
Figures
References
LinkOut - more resources
Full Text Sources
