

Estradiol and progesterone from pregnancy to postpartum: a longitudinal latent class analysis
- PMID: 39444825
- PMCID: PMC11496150
- DOI: 10.3389/fgwh.2024.1428494
Estradiol and progesterone from pregnancy to postpartum: a longitudinal latent class analysis
Abstract
Introduction: During the peripartum, women undergo significant hormonal changes that are crucial for fetal development and a healthy pregnancy and postpartum period for mother and infant. Although several studies have determined healthy norm ranges of estradiol and progesterone, there are discrepancies among the reports, rendering it unclear which hormone levels are linked to adverse health outcomes. To account for the impact of sex steroid patterns on health outcomes in mothers and children, a longitudinal assessment of different parameters is needed.
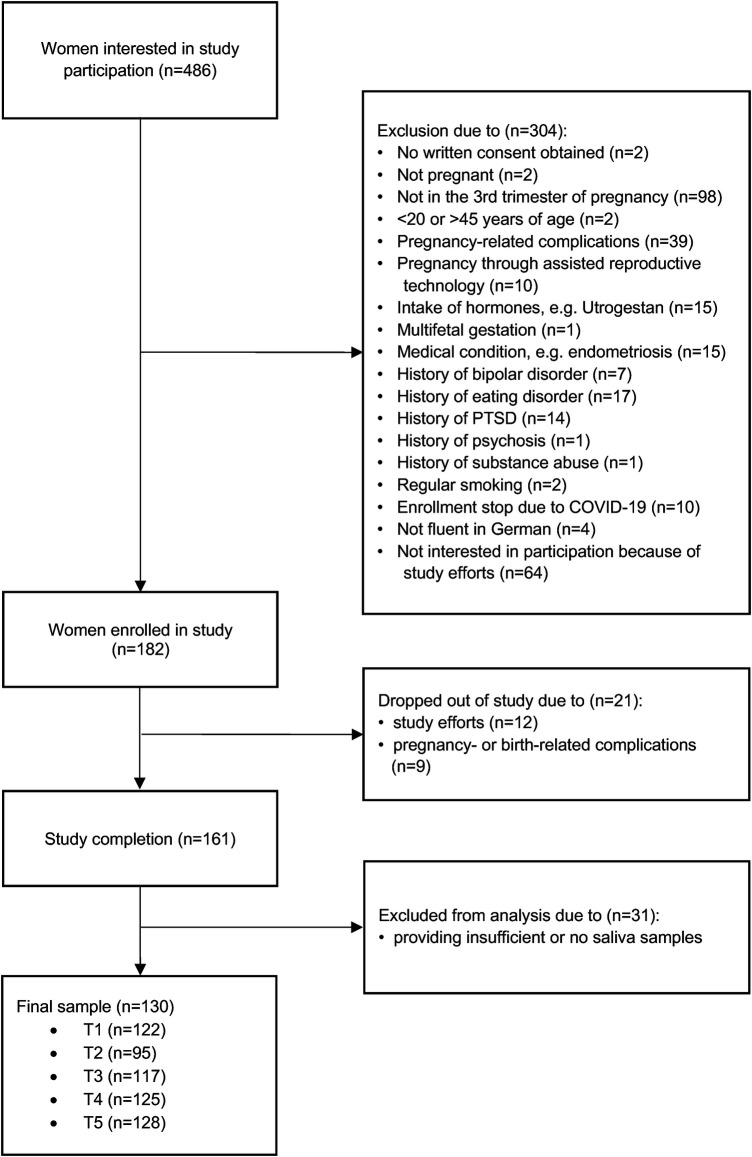
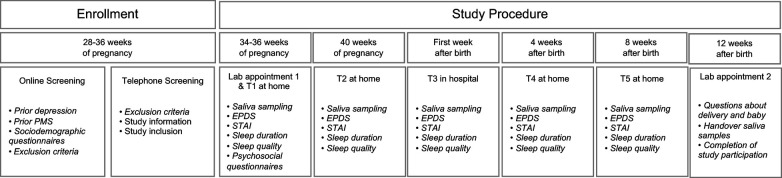
Materials and methods: We longitudinally assessed a cohort of 130 women over five months during pregnancy and postpartum. The women provided saliva samples and completed psychosocial questionnaires. Hormone analyses were conducted using enzyme-linked immunosorbent assay (ELISA). Different parameters of estradiol and progesterone were analyzed and evaluated in relation to psychometric variables. To examine the presence of heterogenous hormonal trajectories in the peripartum, we applied group-based trajectory modelling as a special case of latent-class group analysis.
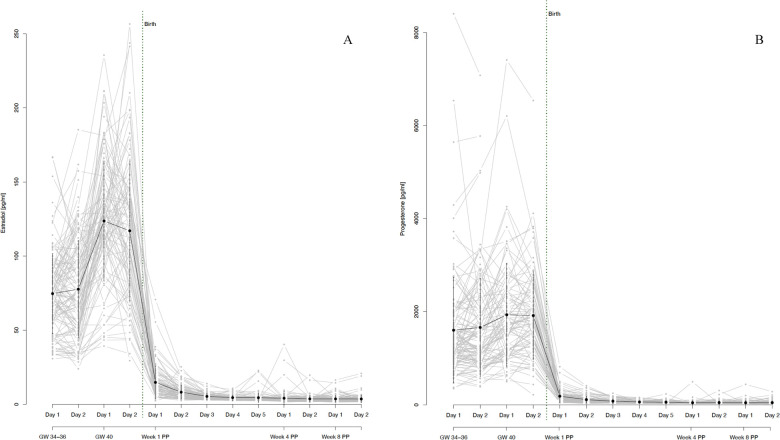
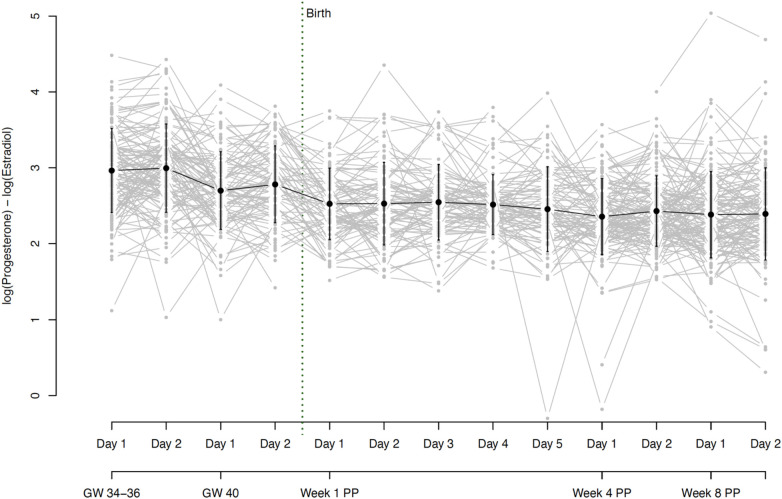
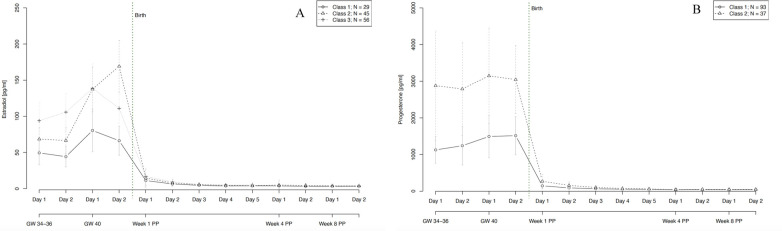
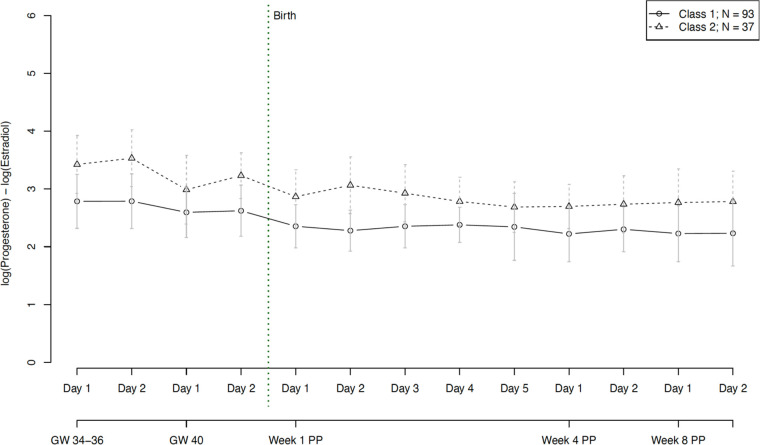
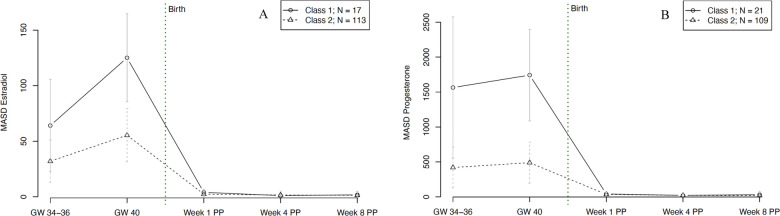
Results: Estradiol and progesterone levels rose towards the end of pregnancy and dropped sharply after birth, with considerable individual variation, particularly during pregnancy. However, their ratio remained stable. We identified three estradiol trajectory subgroups and two progesterone subgroups. Age influenced progesterone levels, with older pregnant women having higher levels than younger women. Anxiety and depressive symptoms had a predictive value for trajectories of specific subgroups of women. The study also revealed two distinct subgroups regarding the course of estradiol and progesterone fluctuations as well as their ratio.
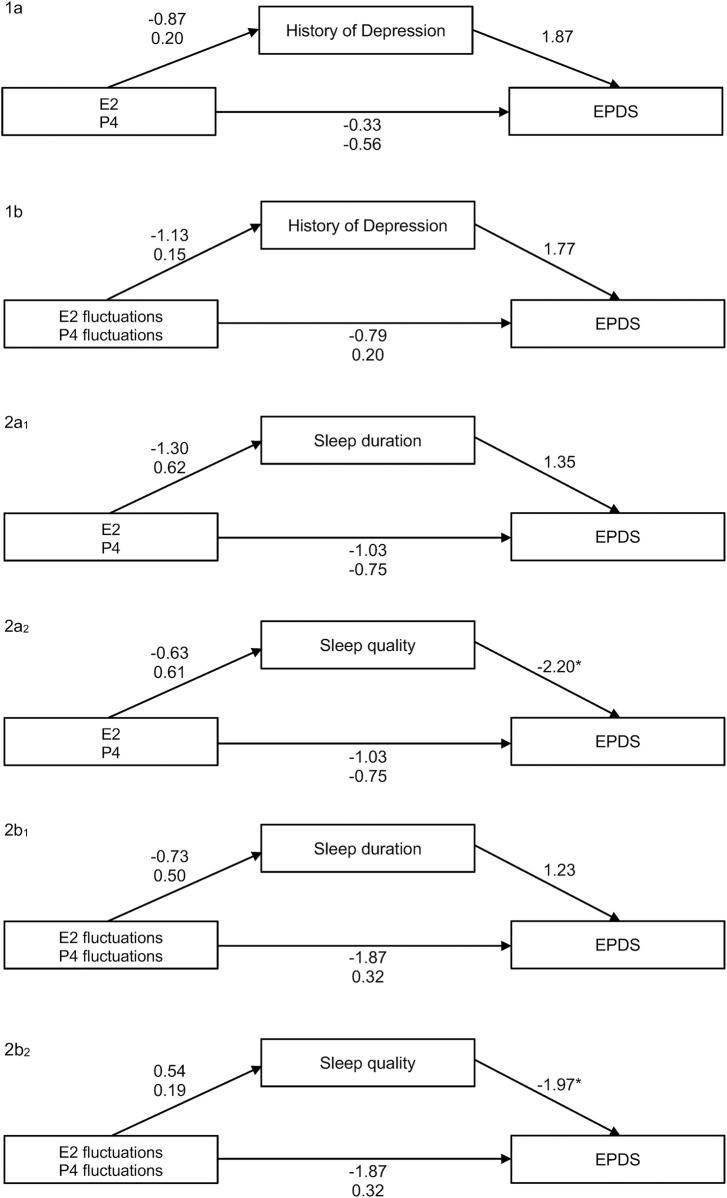
Conclusion: This study provides insights into the course and fluctuation of salivary estradiol and progesterone levels among healthy women during the peripartum period, highlighting significant variations in hormone levels but stability in their ratio during this time. The finding of distinct sex steroid courses in the peripartum is new and suggests the need for further research to explore their impact on health outcomes. Our preliminary results suggest that hormonal fluctuations at the end of pregnancy appear to be a normal occurrence and might even be a protective factor for associated psychological symptoms and sleep disturbances in women.
Keywords: estradiol; hormones; latent-class group analysis; peripartum; postpartum; pregnancy; progesterone; sex steroids.
© 2024 Dukic, Johann, Henninger and Ehlert.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Allopregnanolone and mood in the peripartum: a longitudinal assessment in healthy women.Front Behav Neurosci. 2024 Nov 21;18:1499416. doi: 10.3389/fnbeh.2024.1499416. eCollection 2024. Front Behav Neurosci. 2024. PMID: 39640510 Free PMC article.
-
Longitudinal Course of Sex Steroids From Pregnancy to Postpartum.Endocrinology. 2023 Jun 26;164(8):bqad108. doi: 10.1210/endocr/bqad108. Endocrinology. 2023. PMID: 37450580 Free PMC article. Review.
-
Steroid Hormone Secretion Over the Course of the Perimenopause: Findings From the Swiss Perimenopause Study.Front Glob Womens Health. 2021 Dec 14;2:774308. doi: 10.3389/fgwh.2021.774308. eCollection 2021. Front Glob Womens Health. 2021. PMID: 34970652 Free PMC article.
-
Trajectories of reproductive transition phase mood disorder from pregnancy to postpartum: A Swiss longitudinal study.Womens Health (Lond). 2023 Jan-Dec;19:17455057221147391. doi: 10.1177/17455057221147391. Womens Health (Lond). 2023. PMID: 36748405 Free PMC article.
-
[GABAergic approach of postpartum depression: A translational review of literature].Encephale. 2020 Apr;46(2):123-134. doi: 10.1016/j.encep.2019.09.007. Epub 2019 Nov 22. Encephale. 2020. PMID: 31767256 French.
Cited by
-
Rumination, dyadic coping and parenting sense of competence in couples transitioning to parenthood during puerperium: a longitudinal study protocol.BMJ Open. 2025 Aug 10;15(8):e106214. doi: 10.1136/bmjopen-2025-106214. BMJ Open. 2025. PMID: 40784771 Free PMC article.
-
The complex interaction between oestrogen receptor genes, oestradiol, and perinatal mood.Dialogues Clin Neurosci. 2025 Dec;27(1):24-33. doi: 10.1080/19585969.2025.2482126. Epub 2025 Mar 21. Dialogues Clin Neurosci. 2025. PMID: 40114582 Free PMC article.
-
Association between the number of pregnancies and hearing loss: NHANES 1999-2018.BMC Public Health. 2025 May 22;25(1):1891. doi: 10.1186/s12889-025-23052-0. BMC Public Health. 2025. PMID: 40405121 Free PMC article.
References
-
- Tal R, Taylor HS. Endocrinology of pregnancy. In: Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, de Herder WW, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc. (2000). Bookshelf ID: NBK278962.
LinkOut - more resources
Full Text Sources