

Lung ultrasound score for the assessment of lung aeration in ARDS patients: comparison of two approaches
- PMID: 39444846
- PMCID: PMC11497101
- DOI: 10.1055/a-2421-8709
Lung ultrasound score for the assessment of lung aeration in ARDS patients: comparison of two approaches
Abstract
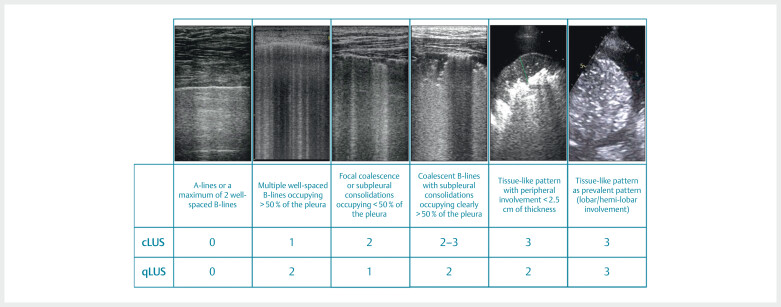
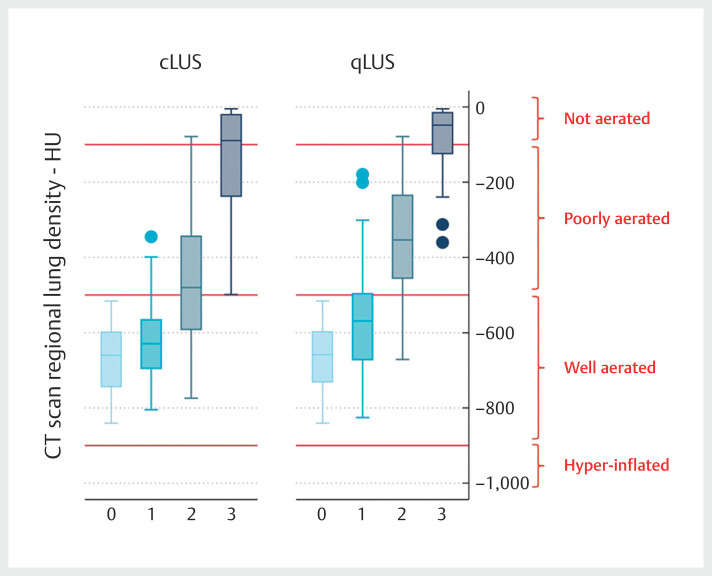
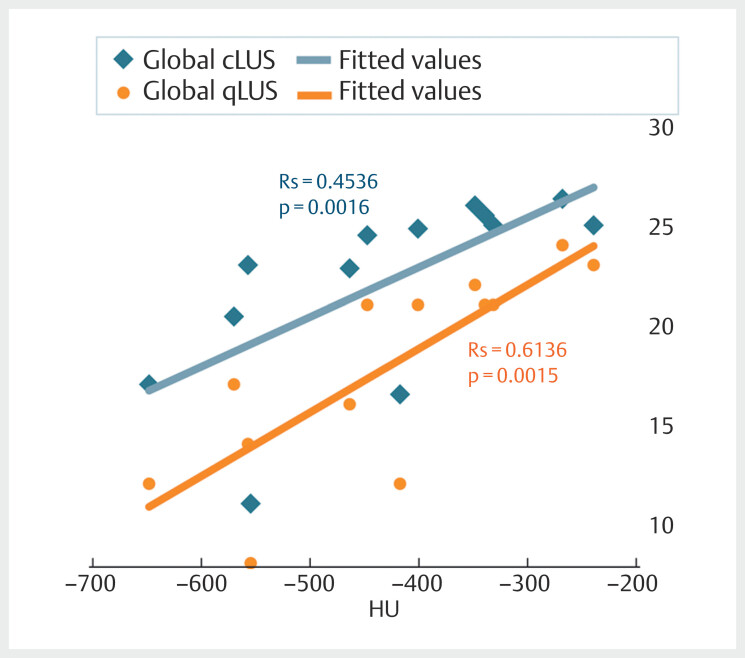
Purpose A 4-step lung ultrasound (LUS) score has been previously used to quantify lung density. We compared 2 versions of this scoring system for distinguishing severe from moderate loss of aeration in ARDS: coalescence-based score (cLUS) vs. quantitative-based score (qLUS - >50% pleura occupied by artefacts). Materials and Methods We compared qLUS and cLUS to lung density measured by quantitative CT scan in 12 standard thoracic regions. A simplified approach (1 scan per region) was compared to an extensive one (regional score computed as the mean of all relevant intercostal space scores). Results We examined 13 conditions in 7 ARDS patients (7 at PEEP 5, 6 at PEEP 15 cmH2O-156 regions, 398 clips). Switching from cLUS to qLUS resulted in a change in interpretation in 117 clips (29.4%, 1-point reduction) and in 41.7% of the regions (64 decreases (range 0.2-1), 1 increase (0.2 points)). Regional qLUS showed very strong correlation with lung density (rs=0.85), higher than cLUS (rs=0.79; p=0.010). The agreement with CT classification in well aerated, poorly aerated, and not aerated tissue was moderate for cLUS (agreement 65.4%; Cohen's K coefficient 0.475 (95%CI 0.391-0.547); p<0.0001) and substantial for qLUS (agreement 81.4%; Cohen's K coefficient 0.701 (95%CI 0.653-0.765), p<0.0001). The agreement between single spot and extensive approaches was almost perfect (cLUS: agreement 89.1%, Cohen's kappa coefficient 0.840 (95%CI 0.811-0.911), p<0.0001; qLUS: agreement 86.5%, Cohen's kappa coefficient 0.819 (95%CI 0.761-0.848), p<0.0001). Conclusion A LUS score based on the percentage of occupied pleura performs better than a coalescence-based approach for quantifying lung density. A simplified approach performs as well as an extensive one.
Keywords: lung aeration; lung density; lung monitoring; lung ultrasound score; quantitative lung ultrasound.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Conflict of Interest FM received fees for lectures from GE Healthcare, Hamilton Medical, SEDA SpA, outside the present work. SM received fees for lectures from GE Healthcare, outside the present work. A research agreement is active between University of Pavia and Hamilton Medical. The other authors declare no conflict of interest.
Figures
References
-
- Soldati G, Inchingolo R, Smargiassi A, Sher S, Nenna R, Inchingolo C D, Valente S. Ex vivo lung sonography: morphologic-ultrasound relationship. Ultrasound Med Biol. 2012;38:1169–1179. - PubMed
-
- Chiumello D, Mongodi S, Algieri I et al. Assessment of Lung Aeration and Recruitment by CT Scan and Ultrasound in Acute Respiratory Distress Syndrome Patients*. Crit Care Med. 2018;46:1761–1768. - PubMed
-
- Mojoli F, Bouhemad B, Mongodi S, Lichtenstein D. Lung Ultrasound for Critically Ill Patients. Am J Respir Crit Care Med. 2019;199:701–714. - PubMed