

The role of wedge resection and lymph node examination in stage IA lung carcinoid tumors
- PMID: 39444868
- PMCID: PMC11494563
- DOI: 10.21037/jtd-24-745
The role of wedge resection and lymph node examination in stage IA lung carcinoid tumors
Abstract
Background: Current guidelines recommend anatomical resection and mediastinal lymph node resection for stage I to IIIA pulmonary carcinoids (PCs). The role of wedge resection in stage IA PCs remains controversial, previous studies focused on typical carcinoids (TCs) while differentiating histological subtypes preoperatively is not easy. We aimed to study the effect of wedge resection and lymph node examination (LNE) in patients with stage IA PCs.
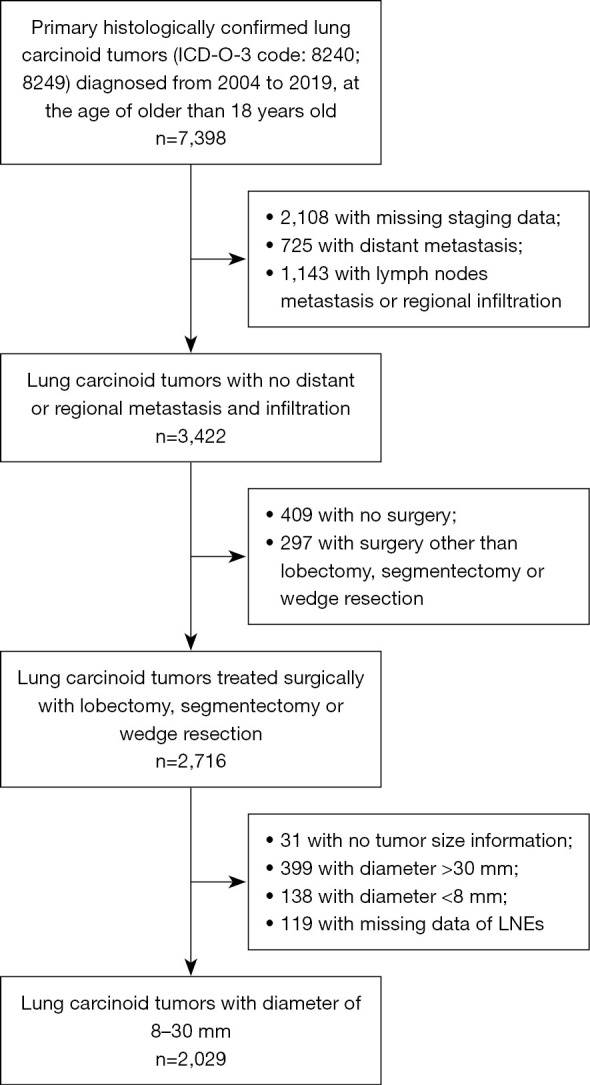
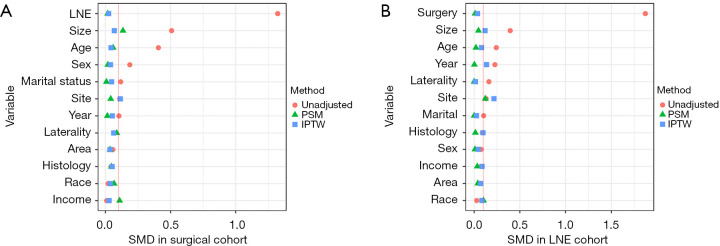
Methods: Patients who underwent anatomical and wedge resection for stage T1N0M0 lung carcinoid tumors between 2004 and 2019 were identified from the Surveillance, Epidemiology, and End Results (SEER) database. Patients were also divided into a non-LNE group and an LNE group. Kaplan-Meier analysis and the log-rank test were used to calculate and compare overall survival (OS). Propensity score matching (PSM) and inverse probability of treatment weighting (IPTW) were used to balance the variables between groups. Univariate and multivariate Cox proportional hazard models were developed to determine prognostic factors.
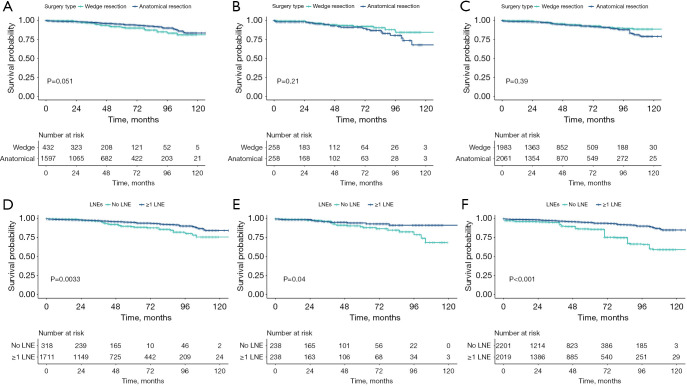
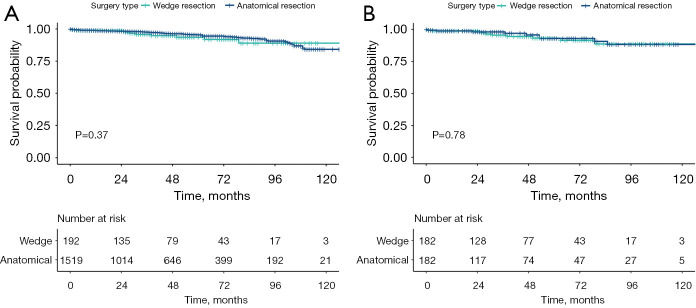
Results: A total of 2,029 patients with bronchopulmonary carcinoid tumors were included in this study, 1,450 underwent lobectomy, 147 underwent segmentectomy and 432 underwent wedge resection. Initially, 5-year survival differed marginally between wedge and anatomical resection (91% vs. 95%, P=0.051), but lost significance after adjustment. LNE improved 5-year survival (95% vs. 89%, P=0.003), and this remained significant after adjustment. In multivariate cox analysis, LNE remained a significant variable while extent of resection was not. This result also remained consistent after adjustment. OS was comparable between wedge resection and anatomical resection when at least 1 lymph node was examined.
Conclusions: For early-stage PC, wedge resection was not inferior to anatomical resection in terms of OS, while LNE significantly increased the survival in both multivariate and matched studies. The relationship between surgical extent and survival in the unadjusted study may be attributed to the lower rate of LNE in wedge resection. Our findings support wedge resection with emphasis on LNE in early-stage PCs.
Keywords: Bronchopulmonary carcinoid; SEER program; anatomical resection; lymph node examination (LNE); wedge resection.
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-745/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- WHO. WHO classification Thoracic tumours. Lyon: IARC Press; 2021.
LinkOut - more resources
Full Text Sources
Miscellaneous