

Lung field-based severity score (LFSS): a feasible tool to identify COVID-19 patients at high risk of progressing to critical disease
- PMID: 39444869
- PMCID: PMC11494559
- DOI: 10.21037/jtd-24-544
Lung field-based severity score (LFSS): a feasible tool to identify COVID-19 patients at high risk of progressing to critical disease
Abstract
Background: Coronavirus disease 2019 (COVID-19) still poses a threat to people's physical and mental health. We proposed a new semi-quantitative visual classification method for COVID-19, and this study aimed to evaluate the clinical usefulness and feasibility of lung field-based severity score (LFSS).
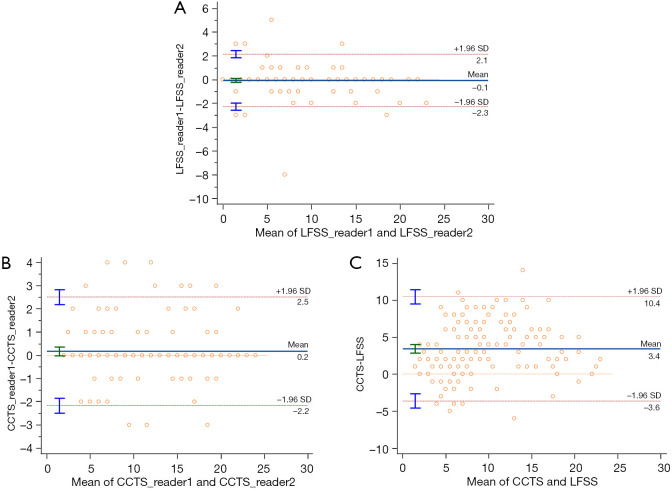
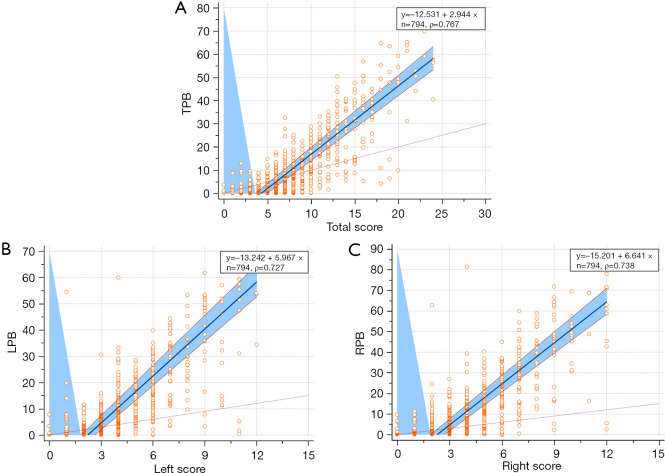
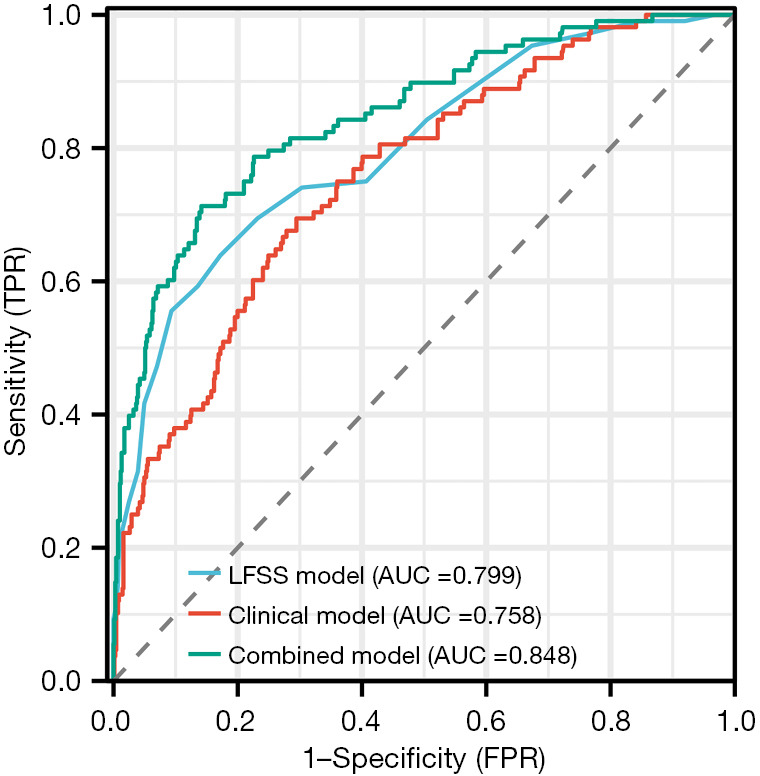
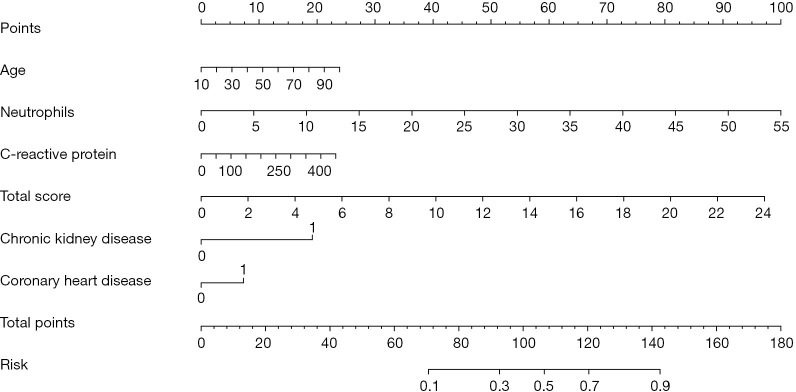
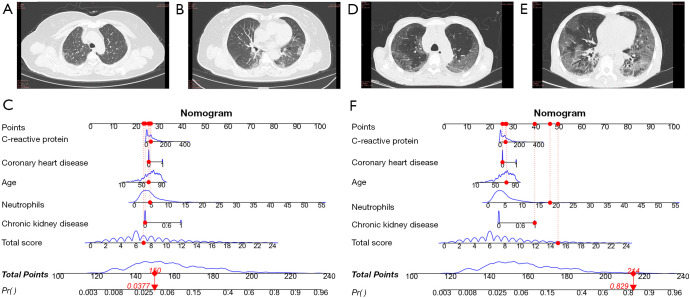
Methods: This retrospective study included 794 COVID-19 patients from two hospitals in China between December 2022 and January 2023. Six lung fields on the axial computed tomography (CT) were defined. LFSS and eighteen clinical characteristics were evaluated. LFSS was based on summing up the parenchymal opacification involving each lung field, which was scored as 0 (0%), 1 (1-24%), 2 (25-49%), 3 (50-74%), or 4 (75-100%), respectively (range of LFSS from 0 to 24). Total pneumonia burden (TPB) was calculated using the U-net model. The correlation between LFSS and TPB was analyzed. After performing logistic regression analysis, an LFSS-based model, clinical-based model and combined model were developed. Receiver operating characteristic curves were used to evaluate and compare the performance of three models.
Results: LFSS, age, chronic liver disease, chronic kidney disease, white blood cell, neutrophils, lymphocytes and C-reactive protein differed significantly between the non-critical and critical group (all P<0.05). There was a strong positive correlation of LFSS and TPB (Pearson correlation coefficient =0.767, P<0.001). The area under curves of LFSS-based model, clinical-based model and combined model were 0.799 [95% confidence interval (CI): 0.770-0.827], 0.758 (95% CI: 0.727-0.788), and 0.848 (95% CI: 0.821-0.872), respectively.
Conclusions: The LFSS derived from chest CT may be a potential new tool to help identify COVID-19 patients at high risk of progressing to critical disease.
Keywords: Coronavirus disease 2019 (COVID-19); computed tomography (CT); prediction.
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-544/coif). The authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials