

Quantitative computed tomography assessment of pulmonary function and compensation after lobectomy and segmentectomy in lung cancer patients
- PMID: 39444877
- PMCID: PMC11494596
- DOI: 10.21037/jtd-24-492
Quantitative computed tomography assessment of pulmonary function and compensation after lobectomy and segmentectomy in lung cancer patients
Abstract
Background: The effect of different surgical methods on postoperative lung function in patients with lung cancer is still inconclusive. The main objective of this study was to compare the effects of video-assisted thoracic surgery (VATS) lobectomy and segmentectomy on postoperative pulmonary function and compensatory changes in patients undergoing lung cancer surgery.
Methods: A total of 120 patients (82 VATS lobectomy, 38 VATS segmentectomy) were assessed for demographic characteristics, baseline pulmonary function, tumor volume, T stage, and histological grade. Postoperative pulmonary function and compensatory changes [percentage of the well-aerated lung (WAL) total (or unilateral) lung volume (LV) (WAL%) and non-operated lung (NOL)] were measured at multiple time points up to 2 years. Logistic regression analysis identified factors associated with WAL% decline after 1 year.
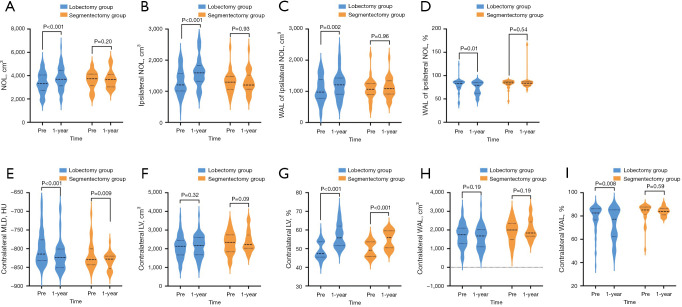
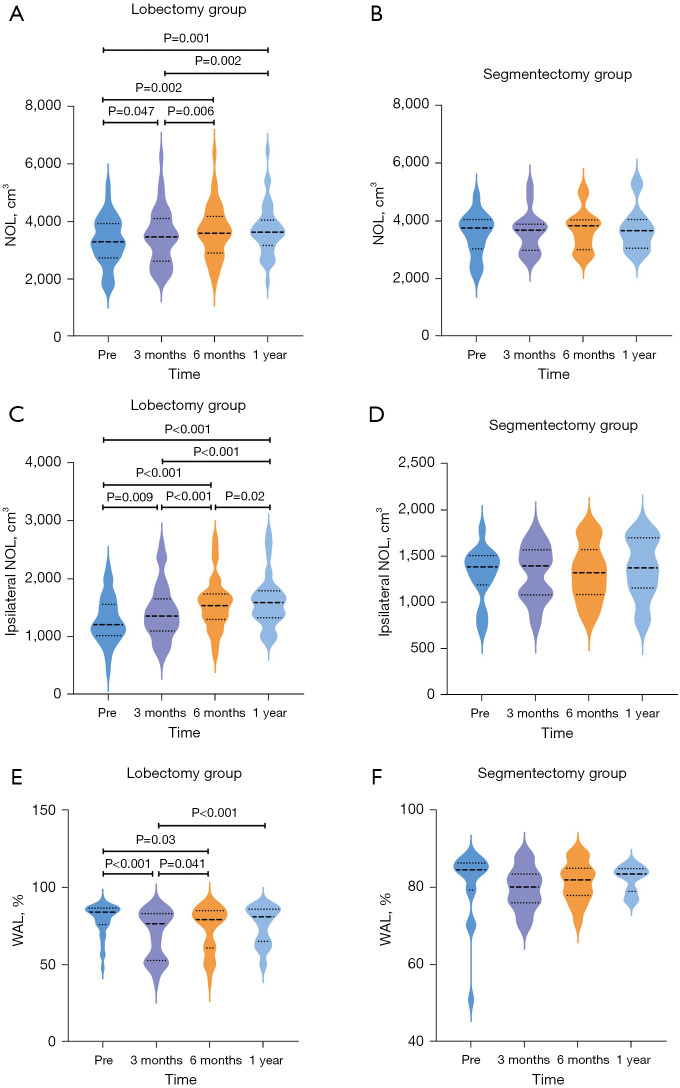
Results: Both VATS lobectomy and segmentectomy led to a decrease in pulmonary function, with no significant difference in the extent of decline between the two groups (all P>0.05). Lobectomy triggered a more pronounced compensatory response, characterized by increased ipsilateral NOL volume over time. Segmentectomy induced minimal compensatory changes and had a minimal impact on pulmonary function. Factors associated with decreased pulmonary ventilation after 1 year differed between the lobectomy and segmentectomy groups. In the lobectomy group, a higher preoperative WAL% of ipsilateral NOL [odds ratio (OR) =1.073; 95% confidence interval (CI): 1.017-1.133; P=0.01] was associated with a higher risk of decline in pulmonary function, whereas in the segmentectomy group, the only influencing factor was the preoperative contralateral mean lung density (MLD) (OR =0.932; 95% CI: 0.884-0.984; P=0.01).
Conclusions: Both lobectomy and segmentectomy after lung cancer surgery result in a decrease in WAL%, with lobectomy demonstrating a stronger pulmonary compensatory capacity. The application of quantitative computed tomography (CT) has shown significant value in predicting postoperative pulmonary function preservation and compensatory changes, providing strong support for personalized surgical decision-making.
Keywords: VATS segmentectomy; Video-assisted thoracic surgery lobectomy (VATS lobectomy); compensatory changes; lung cancer surgery; postoperative pulmonary function.
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-492/coif). S.G. reports that he is an employee of Philips Healthcare. The other authors have no conflicts of interest to declare.
Figures
References
-
- Brunelli A, Kim AW, Berger KI, et al. Physiologic evaluation of the patient with lung cancer being considered for resectional surgery: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013;143:e166S-90S. - PubMed
LinkOut - more resources
Full Text Sources