

The development and validation of a prognostic prediction modeling study in acute myocardial infarction patients after percutaneous coronary intervention: hemorrhea and major cardiovascular adverse events
- PMID: 39444902
- PMCID: PMC11494537
- DOI: 10.21037/jtd-24-1362
The development and validation of a prognostic prediction modeling study in acute myocardial infarction patients after percutaneous coronary intervention: hemorrhea and major cardiovascular adverse events
Abstract
Background: Percutaneous coronary intervention (PCI) is one of the most important diagnostic and therapeutic techniques in cardiology. At present, the traditional prediction models for postoperative events after PCI are ineffective, but machine learning has great potential in identification and prediction of risk. Machine learning can reduce overfitting through regularization techniques, cross-validation and ensemble learning, making the model more accurate in predicting large amounts of complex unknown data. This study sought to identify the risk of hemorrhea and major adverse cardiovascular events (MACEs) in patients after PCI through machine learning.
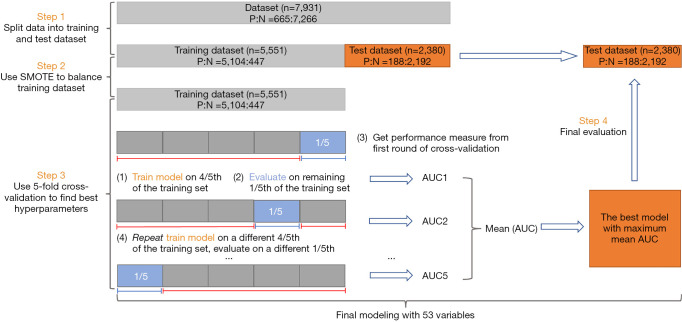
Methods: The entire study population consisted of 7,931 individual patients who underwent PCI at Jiangsu Provincial Hospital and The Affiliated Wuxi Second People's Hospital from January 2007 to January 2022. The risk of postoperative hemorrhea and MACE (including cardiac death and in-stent restenosis) was predicted by 53 clinical features after admission. The population was assigned to the training set and the validation set in a specific ratio by simple randomization. Different machine learning algorithms, including eXtreme Gradient Boosting (XGBoost), random forest (RF), and deep learning neural network (DNN), were trained to build prediction models. A 5-fold cross-validation was applied to correct errors. Several evaluation indexes, including the area under the receiver operating characteristic (ROC) curve (AUC), accuracy (Acc), sensitivity (Sens), specificity (Spec), and net reclassification improvement (NRI), were used to compare the predictive performance. To improve the interpretability of the model and identify risk factors individually, SHapley Additive exPlanation (SHAP) was introduced.
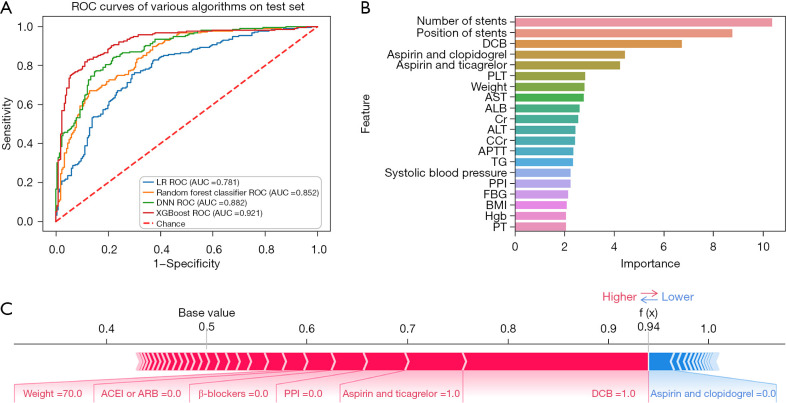
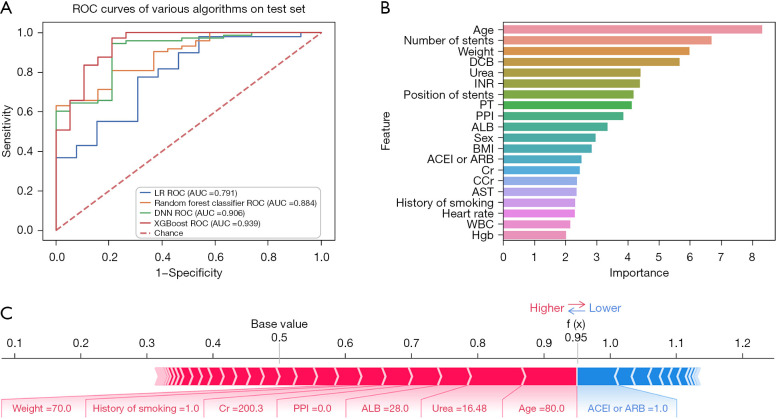
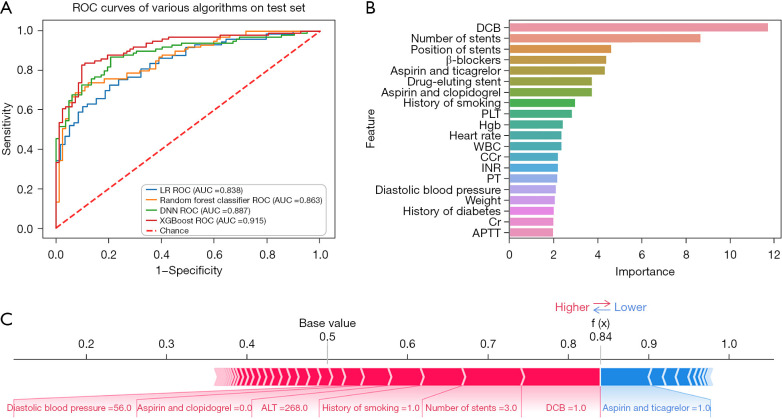
Results: In this study, 306 patients (3.9%) experienced hemorrhea, 107 patients (1.3%) experienced cardiac death, and 218 patients (2.7%) developed in-stent restenosis. In the training set and validation set, except for previous PCI and statins, there were no significant differences. XGBoost was observed to be the best predictor of every event, namely hemorrhea [AUC: 0.921, 95% confidence interval (CI): 0.864-0.978, Acc: 0.845, Sens: 0.851, Spec: 0.837 and NRI: 0.140], cardiac death (AUC: 0.939, 95% CI: 0.903-0.975, Acc: 0.914, Sens: 0.950, Spec: 0.800 and NRI: 0.148), and in-stent restenosis (AUC: 0.915; 95% CI: 0.863-0.967, Acc: 0.834, Sens: 0.778, Spec: 0.902 and NRI: 0.077). SHAP showed that the number of stents had the greatest influence on hemorrhea, while age and drug-coated balloon were the main factors in cardiogenic death and stent restenosis (all P<0.05).
Conclusions: The XGBoost model (machine learning) performed better than the traditional logistic regression model in identifying hemorrhea and MACE after PCI. Machine learning models can be used as a tool for risk prediction. The machine learning model described in this study can personalize the prediction of hemorrhea and MACE after PCI for specific patients, helping clinicians adjust intervenable features.
Keywords: Acute myocardial infarction (AMI); eXtreme Gradient Boosting (XGBoost); machine learning; major adverse cardiovascular events (MACEs); percutaneous coronary intervention (PCI).
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-1362/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Machine learning-based predictive models for perioperative major adverse cardiovascular events in patients with stable coronary artery disease undergoing noncardiac surgery.Comput Methods Programs Biomed. 2025 Mar;260:108561. doi: 10.1016/j.cmpb.2024.108561. Epub 2024 Dec 13. Comput Methods Programs Biomed. 2025. PMID: 39708562
-
Risk Prediction of Major Adverse Cardiovascular Events Occurrence Within 6 Months After Coronary Revascularization: Machine Learning Study.JMIR Med Inform. 2022 Apr 20;10(4):e33395. doi: 10.2196/33395. JMIR Med Inform. 2022. PMID: 35442202 Free PMC article.
-
Application of machine learning model in predicting the likelihood of blood transfusion after hip fracture surgery.Aging Clin Exp Res. 2023 Nov;35(11):2643-2656. doi: 10.1007/s40520-023-02550-4. Epub 2023 Sep 21. Aging Clin Exp Res. 2023. PMID: 37733228 Clinical Trial.
-
Predicting Major Adverse Cardiovascular Events in Acute Coronary Syndrome: A Scoping Review of Machine Learning Approaches.Appl Clin Inform. 2022 May;13(3):720-740. doi: 10.1055/a-1863-1589. Epub 2022 May 26. Appl Clin Inform. 2022. PMID: 35617971 Free PMC article.
-
Methodological Review of Classification Trees for Risk Stratification: An Application Example in the Obesity Paradox.Nutrients. 2025 May 31;17(11):1903. doi: 10.3390/nu17111903. Nutrients. 2025. PMID: 40507172 Free PMC article. Review.
Cited by
-
Correlation of blood lipids, glucose, and inflammatory indices with the occurrence and prognosis of lesion complexity in unstable angina, a retrospective cohort study.J Thorac Dis. 2025 Jan 24;17(1):413-428. doi: 10.21037/jtd-2024-2122. Epub 2025 Jan 22. J Thorac Dis. 2025. PMID: 39975718 Free PMC article.
References
-
- Nishihira K, Kuriyama N, Kadooka K, et al. Outcomes of Elderly Patients With Acute Myocardial Infarction and Heart Failure Who Undergo Percutaneous Coronary Intervention. Circ Rep 2022;4:474-81. 10.1253/circrep.CR-22-0048 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous