

Signature stemmed from two transcription factor families determines histological fate and regulates immune infiltration in patients with lung cancer
- PMID: 39444905
- PMCID: PMC11494554
- DOI: 10.21037/jtd-24-733
Signature stemmed from two transcription factor families determines histological fate and regulates immune infiltration in patients with lung cancer
Abstract
Background: Earlier research has reported that transcription factors play a crucial role in the anti-tumorigenic immune response of lung cancer patients. The aim of this study is to determine the relationship between post-translational modifications of transcription factors and histological fate and patient prognosis.
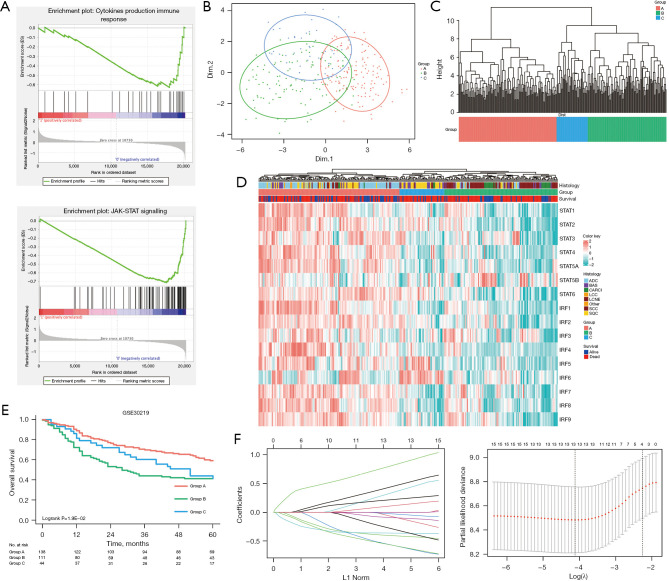
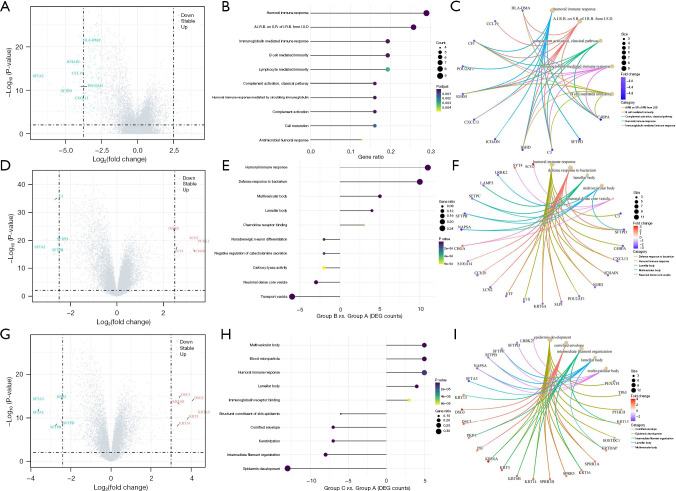
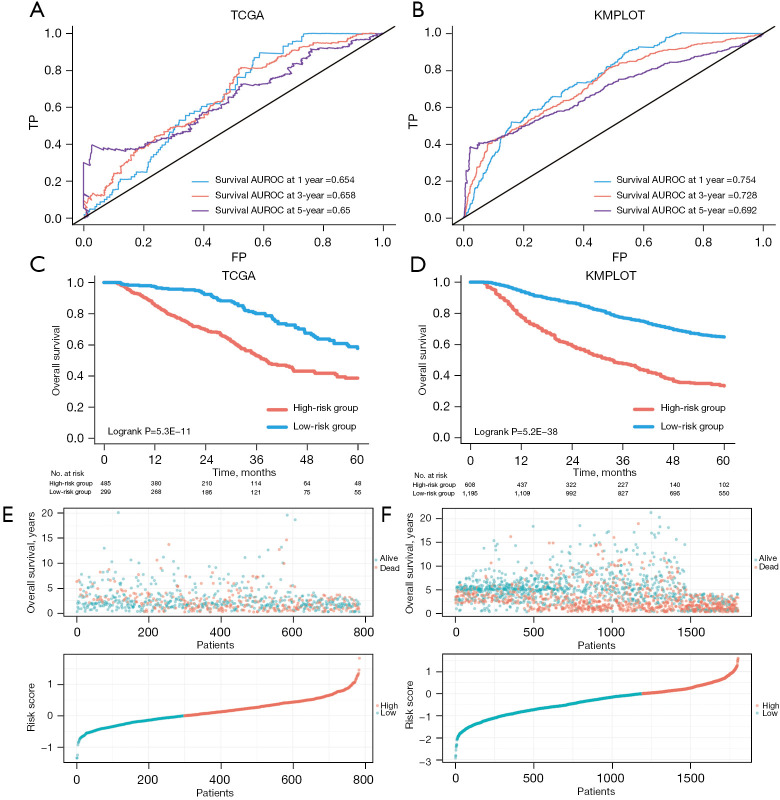
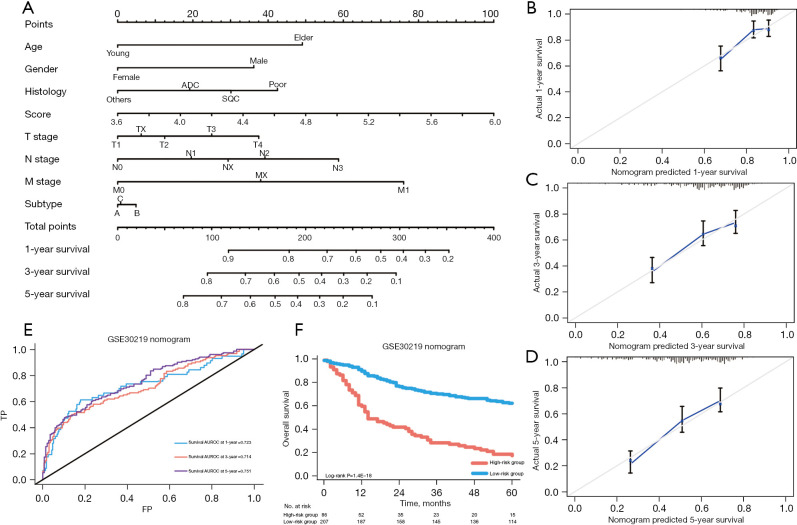
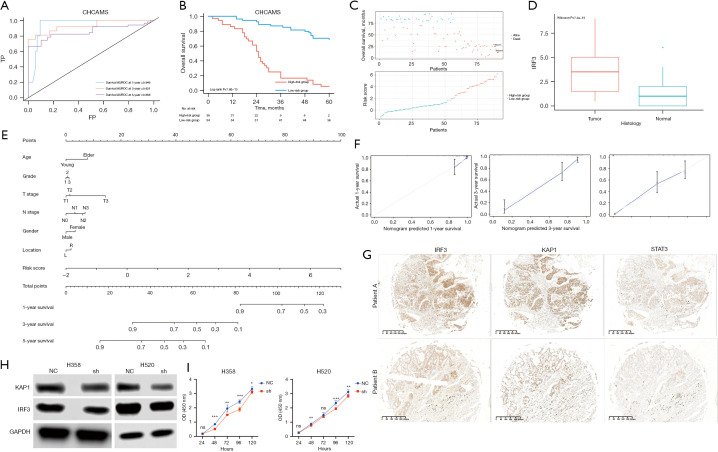
Methods: Based on the information of 293 lung cancer patients in the Gene Expression Omnibus (GEO) database, differentially expressed genes (DEGs) related to the interferon regulatory factor (IRF) and signal transducer and activator of transcription (STAT) families between patients experiencing early death and those with long-term survival were identified and characterized. A survival prediction model was established by incorporating 7 STAT genes and 9 IRF genes into the least absolute shrinkage and selection operator (LASSO) algorithm. Gene Ontology (GO) enrichment analysis indicated that these two transcription factor families can govern lung cancer tissue differentiation and predict patient prognosis. Moreover, the Cox proportional hazards regression model was applied to select the genes with the highest predictive capability to construct a gene-based signature. Lastly, the data of 1,803 and 784 lung cancer patients from the Kaplan-Meier plotter (KMPLOT) and The Cancer Genome Atlas (TCGA) databases were used to evaluate the accuracy and sensitivity of the model.
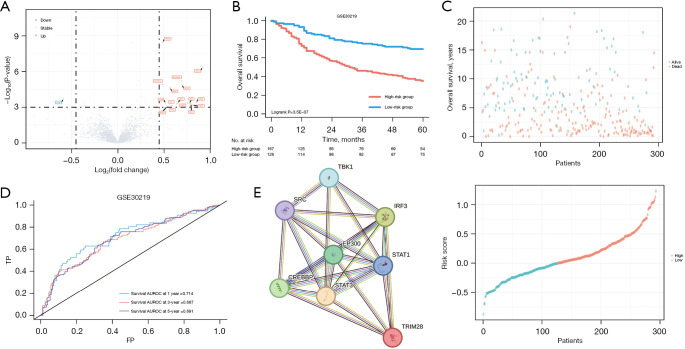
Results: Based on the minimum criterion, TRIM28, IRF3, and STAT3 were employed to generate the prognostic model. The 1-, 3-, and 5-year area under the curve (AUC) values of the three-gene-based signature showed consistent results, signifying that the model had excellent accuracy and sensitivity in predicting overall survival (OS) for patients with lung cancer. Finally, the three-gene signature and tumor-node-metastasis (TNM) staging system were combined to construct a nomogram for evaluating the OS of lung cancer patients. TRIM28 may affect the stability of IRF3. Encouragingly, the predicted OS was highly consistent with the observed OS in multiple cohorts.
Conclusions: Taken together, these findings implied that the predictive model based on the three-gene signature showed robust discriminatory performance.
Keywords: Lung cancer; biomarkers; immunology; transcriptomics.
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-733/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018;391:1023-75. 10.1016/S0140-6736(17)33326-3 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous