

Sex-related disparities in aortic stenosis from disease awareness to treatment: a state-of-the-art review
- PMID: 39444914
- PMCID: PMC11494558
- DOI: 10.21037/jtd-24-406
Sex-related disparities in aortic stenosis from disease awareness to treatment: a state-of-the-art review
Abstract
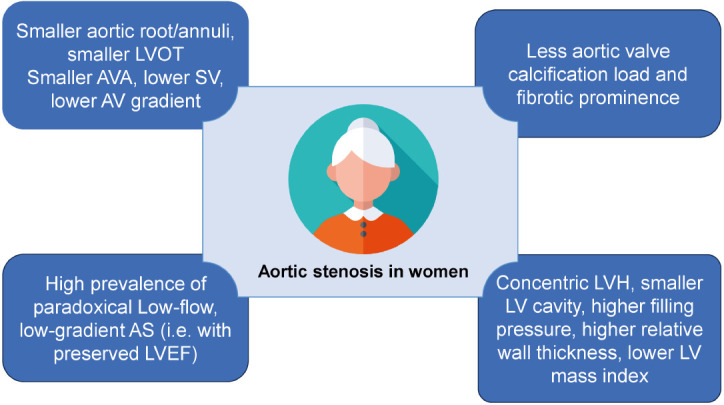
This state-of-the-art review aimed to synthesize evidence from various sex-stratified studies on aortic stenosis (AS), focusing on the difference in clinical presentation, anatomical characteristics, pathophysiology, and management of AS. In comparison to men, women with AS are present at later stages, are older, more symptomatic, frailer, and exhibit higher operative risk [Society of Thoracic Surgeons (STS) score]. Women tend to have smaller aortic valve (AV) areas and left ventricular (LV) outflow tract, leading to lower stroke volumes (SVs) than men and have a higher prevalence of paradoxical, low-flow, low-gradient AS. In women, chronic pressure overload due to AS results in concentric LV remodelling and hypertrophy, characterized by reduced LV cavities, higher filling pressures, lower wall stress, and more diastolic dysfunction. Conversely, men exhibit more dilated eccentric LV remodelling and hypertrophy. AVs in women are less calcified but more fibrotic. Moreover, women are often underdiagnosed, have severity underestimated, and experience delays or receive fewer referrals for AV replacement (AVR). However, women tend to benefit from transcatheter AVR (TAVR) with a long-term survival advantage over men, although the incidence of vascular complications and bleeding events in 30 days after TAVR is higher in women. Surgical AVR (SAVR) in women has high operative risk, is technically demanding and has poorer outcomes with increased mortality at 30 days compared to men. According to the STS score and EuroSCORE, the female sex itself is considered a risk factor for SAVR. Therefore, addressing sex-related disparities in AS and increasing awareness among physicians promises improved diagnosis and treatment, facilitating equitable care and the development of sex-specific personalized medicine.
Keywords: Aortic stenosis (AS); sex differences; surgical aortic valve replacement (SAVR); transcatheter aortic valve replacement (TAVR); women.
2024 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-24-406/coif). C.A. reports that she received speaker honoraria and has received travel support from Edwards Lifesciences, Medtronic and Boston. S.B. received speaker honoraria from Abbott Vascular, Boston Scientific, Edwards Lifesciences, and Medtronic. IPPMed, Cloppenburg, Germany, represented by P.B., has received honoraria (or research funding) for consultancy and medical writing from Edwards Lifesciences. V.D. received honoraria for lectures, presentations, and speakers from Abbott Vascular, Edwards Lifesciences, GE Healthcare, JenaValve, Medtronic, and Novartis Products & Features. Also, she received research grants from Philips and consultation fees from Edwards Lifesciences, Novo Nordisk, and MSD. H.E. received honoraria for lectures from Edwards Lifesciences. C.G. was supported by research grants from the Novartis Foundation, Switzerland; GE Healthcare, US; Gerresheimer AG, Switzerland; Bayer Pharmaceuticals, Switzerland; AMGEN, Switzerland; and Advisis AG, Switzerland, outside of the submitted work; has received travel support from Siemens Healthineers, Germany, and Biotronik, Switzerland; and has received speaker’s fees from Sanofi Genzyme, France. C.H. received institutional grant/research support from Abbott, Boston Scientific, Edwards Lifesciences, Medtronic, and Meril; received consultant fees and honoraria from Edwards Lifesciences, Boston Scientific, and Meril. J.K. is an employee of Edwards Lifesciences and owns stocks from that company. P.M. is a scientist working for Edwards Lifesciences. T.K.R. received research support for medical writing from IPPMed, Germany. W.W. received honoraria for lectures, presentations, speakers and travel support from Abbott Vascular, Medtronic, and Edward lifesciences; received research consultancy fees and received payment for participation in data safety monitoring board or advisory board from Medtronic. The authors have no other conflicts of interest to declare.
Figures
Similar articles
-
Outcomes in the Randomized CoreValve US Pivotal High Risk Trial in Patients With a Society of Thoracic Surgeons Risk Score of 7% or Less.JAMA Cardiol. 2016 Nov 1;1(8):945-949. doi: 10.1001/jamacardio.2016.2257. JAMA Cardiol. 2016. PMID: 27541162 Clinical Trial.
-
Surgical aortic valve replacement and left ventricular remodeling: Survival and sex-related differences.Echocardiography. 2021 Jul;38(7):1095-1103. doi: 10.1111/echo.15122. Epub 2021 May 24. Echocardiography. 2021. PMID: 34028878
-
Sex Disparities in the Treatment of Aortic Stenosis and Related Outcomes: An Analysis of the National Inpatient Sample.Cardiology. 2022;147(5-6):557-565. doi: 10.1159/000526255. Epub 2022 Sep 14. Cardiology. 2022. PMID: 36103808
-
Sex-Specific Considerations in Women with Aortic Stenosis and Outcomes After Transcatheter Aortic Valve Replacement.Curr Treat Options Cardiovasc Med. 2018 Jun 19;20(7):52. doi: 10.1007/s11936-018-0651-x. Curr Treat Options Cardiovasc Med. 2018. PMID: 29923126 Review.
-
Time course of the survival advantage of transcatheter over surgical aortic valve replacement: Interplay between sex and patient risk profile.Catheter Cardiovasc Interv. 2019 Nov 1;94(5):746-752. doi: 10.1002/ccd.28124. Epub 2019 Feb 28. Catheter Cardiovasc Interv. 2019. PMID: 30821116
Cited by
-
Understanding Aortic Stenosis and Transcatheter Aortic Valve Replacement in Women.Struct Heart. 2025 May 30;9(7):100666. doi: 10.1016/j.shj.2025.100666. eCollection 2025 Jul. Struct Heart. 2025. PMID: 40704359 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials