

The Effects of Heat Therapy During Immobilization and Rehabilitation on Muscle Atrophy and Strength Loss at Return to Sports in Healthy Humans
- PMID: 39444938
- PMCID: PMC11497528
- DOI: 10.1177/23259671241281727
The Effects of Heat Therapy During Immobilization and Rehabilitation on Muscle Atrophy and Strength Loss at Return to Sports in Healthy Humans
Erratum in
-
Corrigendum to "The Effects of Heat Therapy During Immobilization and Rehabilitation on Muscle Atrophy and Strength Loss at Return to Sports in Healthy Humans".Orthop J Sports Med. 2024 Dec 13;12(12):23259671241307664. doi: 10.1177/23259671241307664. eCollection 2024 Dec. Orthop J Sports Med. 2024. PMID: 39678435 Free PMC article.
Abstract
Background: Animal research suggests that repeated heat exposures may stimulate skeletal muscle protein synthesis and downregulate protein degradation.
Hypothesis: Repeated heat exposures during ankle immobilization and rehabilitation would preserve human muscle strength and mass.
Study design: Controlled laboratory study.
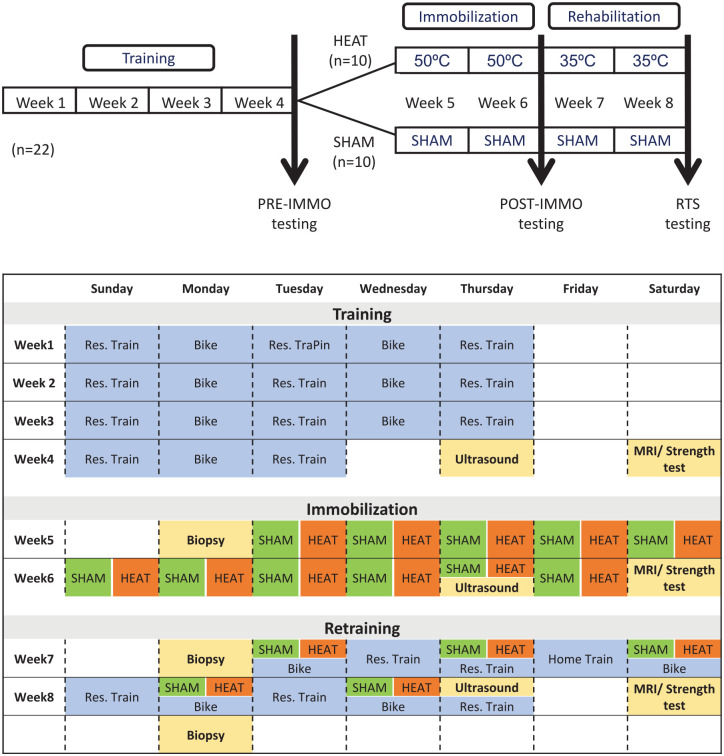
Methods: A total of 20 male participants (age, 33.6 ± 2.8 years; weight, 83.8 ± 9.2 kg; height, 182 ± 6 cm) underwent 4 weeks of supervised training, 2 weeks of single-lower leg immobilization, and 2 weeks of supervised rehabilitation before return to sports (RTS). Participants were split into 2 groups: (1) whole-body heat therapy (HEAT) and (2) sham treatment (SHAM) throughout the immobilization and rehabilitation periods. Measures of muscle strength (isometric and isokinetic), volume (magnetic resonance imaging and ultrasound), and muscle biopsies were obtained preimmobilization, postimmobilization, and at RTS.
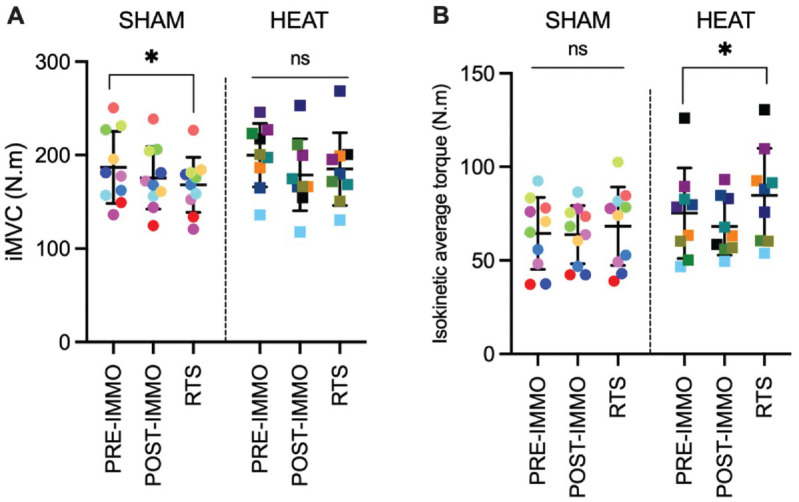
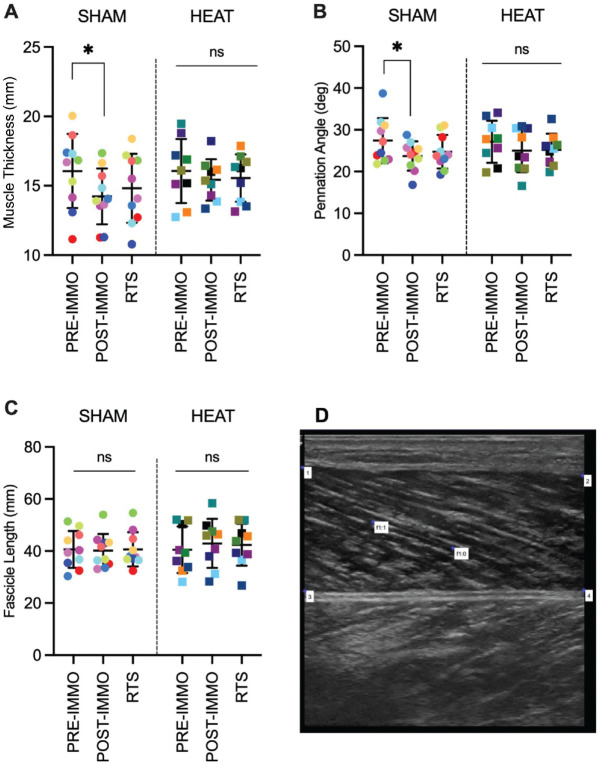
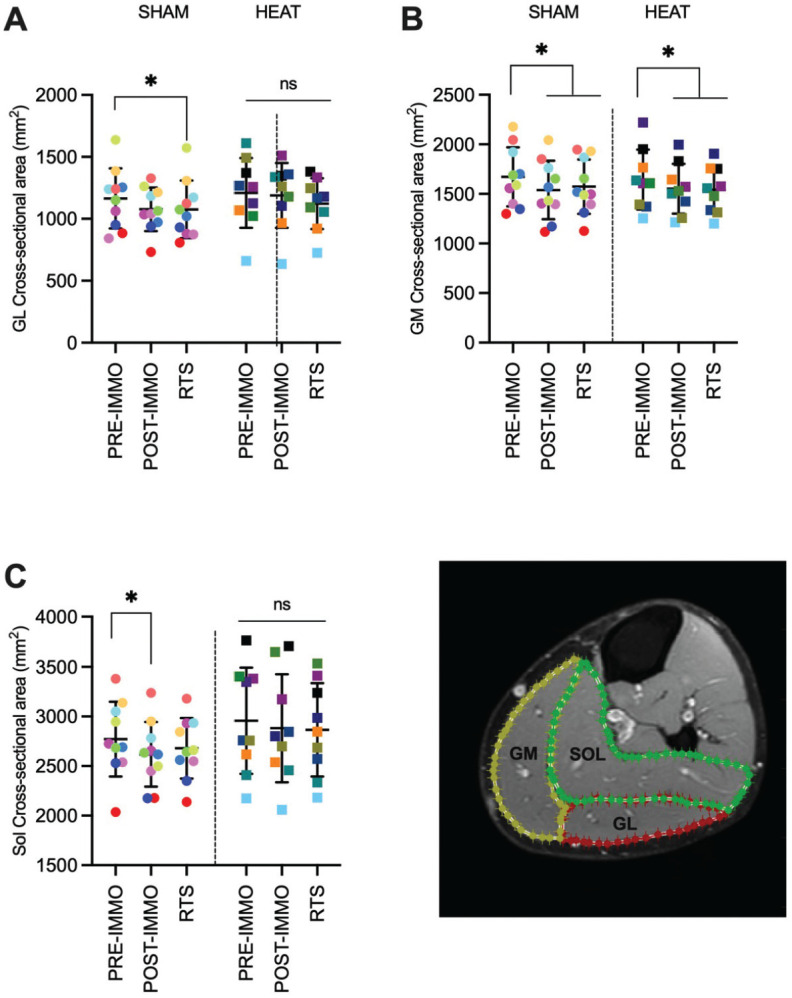
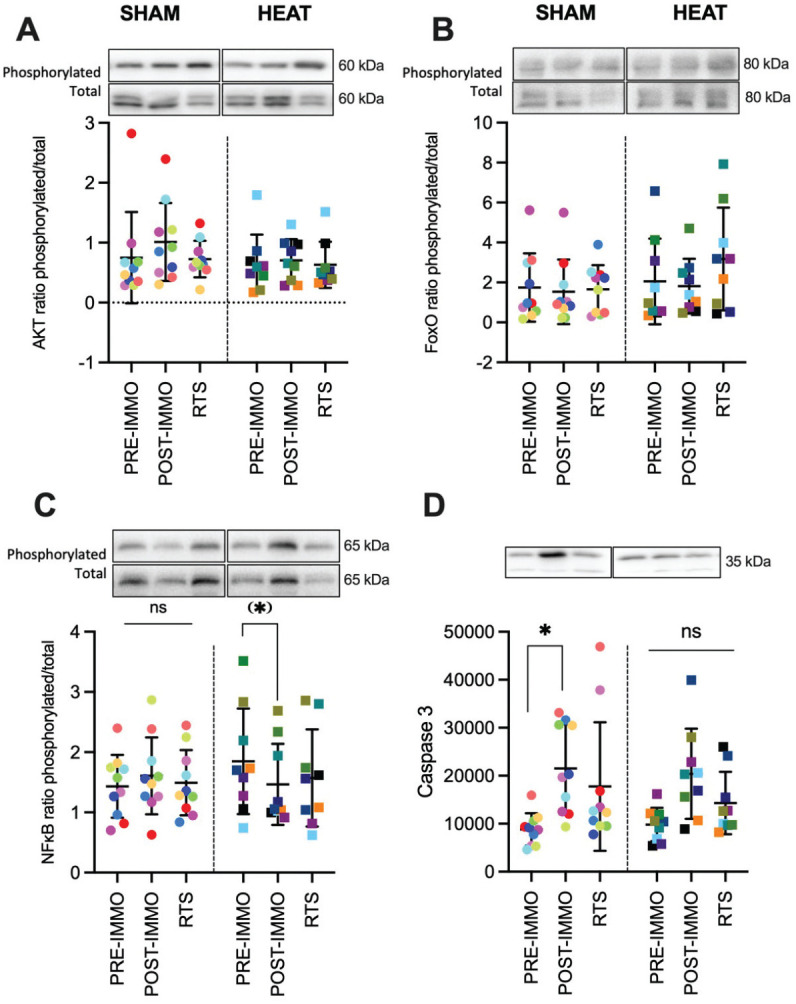
Results: Maximal isometric strength of the plantarflexors was lower at RTS compared with preimmobilization in SHAM (P = .027) but not HEAT (P = .301). Isokinetic strength during a fatigue test was higher at RTS compared with preimmobilization in HEAT (P = .039) but not SHAM (P = .245). Pennation angle and muscle thickness were lower at postimmobilization compared with preimmobilization only in SHAM (P≤ .027). Muscle cross-sectional area decreased in soleus and both gastrocnemius medialis and lateralis (all P≤ .035) in SHAM, but only in gastrocnemius medialis in HEAT. There was a large (d = 0.91) but not significant (P = .054) decrease in the ratio of phosphorylated/total nuclear factor-kappa B (NFκB) from preimmobilization to postimmobilization in HEAT only. There was an increase in phosphorylated fork head box O proteins (FoxO) only in HEAT (P = .034), suggesting a decrease in FoxO activity. Caspase 3 expression increased from preimmobilization to postimmobilization in SHAM only (P = .004).
Conclusion: These results indicate that using heat therapy throughout immobilization and rehabilitation reduces skeletal muscle atrophy and maintains plantarflexor strength in healthy humans. Moreover, heat therapy may lead to the inactivation of the FoxO and NFκB signaling pathways involved in atrophy.
Clinical relevance: Repeated heat exposures should be considered a novel therapeutic intervention to counteract muscle atrophy during immobilization.
Keywords: ankle; athletic training; biologic healing enhancement; muscle injuries; muscle physiology; physical therapy modalities; physical therapy/rehabilitation.
© The Author(s) 2024.
Conflict of interest statement
The authors declare that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
