

Possible clinical and radiological predictors of haemorrhagic transformation in acute stroke patients undergoing dual antiplatelet therapy: a clinical study
- PMID: 39445085
- PMCID: PMC11497499
- DOI: 10.1177/17562864241289735
Possible clinical and radiological predictors of haemorrhagic transformation in acute stroke patients undergoing dual antiplatelet therapy: a clinical study
Abstract
Background: The predictors of intracranial haemorrhagic transformation (HT) in acute ischaemic stroke (AIS) patients undergoing dual antiplatelet therapy (DAPT) are not well known.
Objectives: The aim of this study is to identify the possible clinical and radiological predictors of HT in patients, irrespective of clinical indication for this treatment.
Design: This study is a monocentric cohort retrospective study.
Methods: We enrolled consecutive AIS patients, from our prospective register, admitted to Stroke Unit between June 2021 and June 2023 undergoing DAPT with Acetylsalicylic Acid and Clopidogrel within 72 h from symptoms onset. According to current guidelines, DAPT indication was for patients with a minor stroke, symptomatic intracranial artery stenosis and carotid angioplasty stenting. We collected clinical, demographical and radiological data. We used ABC/2 method to measure stroke volume in magnetic resonance imaging (MRI)/Diffusion-weighted imaging (DWI) sequences performed within 48 h. The primary outcome was the presence of HT at non-contrast brain computed tomography, performed 7 days after commencing DAPT.
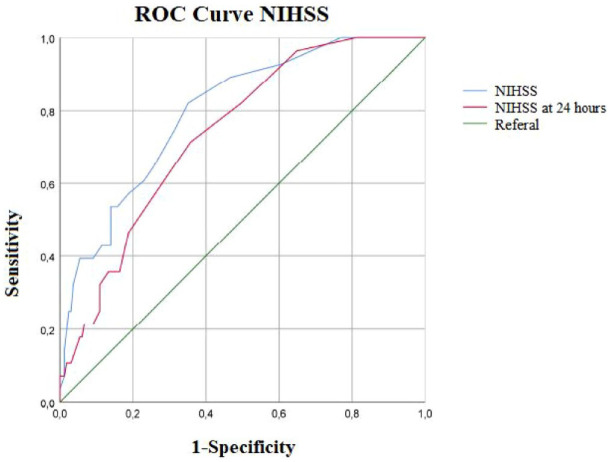
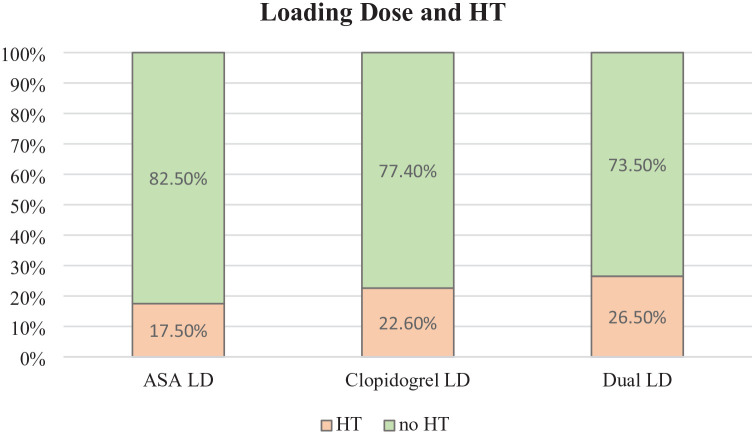
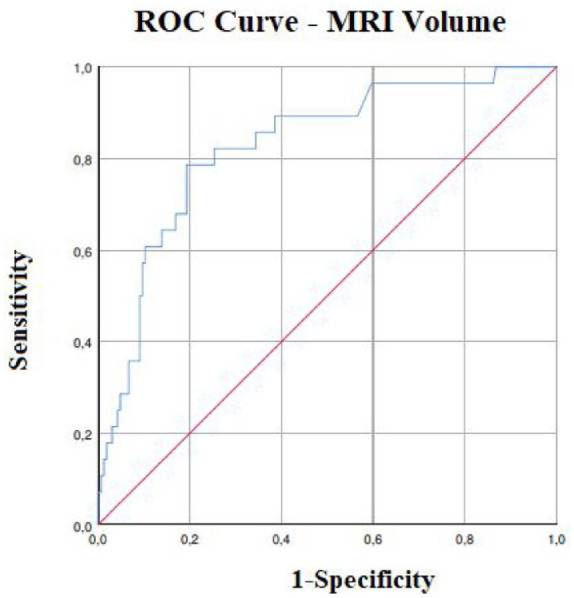
Results: One hundred ninety-four patients were included. Twenty-eight (14.4%) presented HT. Higher NIH Stroke Scale (NIHSS) and MRI/DWI lesion volume related to increased risk of HT (p < 0.001). Reperfusion therapy and mechanical thrombectomy (MT), stent placement and a loading dose (LD) of dual antiplatelet or Clopidogrel were associated with a higher occurrence of HT (p < 0.05). Furthermore, we individuated an NIHSS cut-off value >4 (area under the curve (AUC) 0.80, sensitivity 0.82, specificity 0.65) and a volume cut-off value >8.2 ml (AUC 0.82, sensitivity 0.79, specificity 0.80) associated with an increased risk of HT (respectively, adjusted odds ratio (adj. OR) 6.5, confidence interval (CI) 1.3-32.7, p = 0.024 and adj. OR 11.0, CI 3.1-39.2, p < 0.001).
Conclusion: In clinical practice, MT treatment, antiplatelet LD administration, stent placement and clinical severity may relate to a higher risk of HT in patients with AIS and DAPT in the acute phase. In particular, we found that lesion volume cut-off could help to identify patients at greater risk of HT, regardless of the indication for DAPT.
Keywords: MRI; acute ischaemic stroke; biomarkers; dual antiplatelet therapy; haemorrhagic transformation.
Plain language summary
Possible clinical and radiological features able to predict the risk of haemorrhagic transformation in patients affected by acute cerebral ischemic stroke undergoing treatment with dual antiplatelet, Acid Acetylsalicylic and Clopidogrel This monocentric cohort retrospective study aims to identify predictive factors for haemorrhagic transformation (HT) in patients with acute ischaemic stroke (AIS) and dual antiplatelet therapy (DAPT). DAPT is indicated for minor strokes, symptomatic intracranial artery stenosis and carotid stent placement. Although there are guidelines on this subject, there are some grey areas due to the emergence of new possible uses of DAPT and to a lack of studies addressing some issues (e.g. patients with moderate to severe AIS undergoing DAPT). We selected patients >18 years old from our prospective registry, who were admitted for AIS and started DAPT within 72 hours from the event. We collected clinical and radiological data. All patients underwent brain magnetic resonance imaging (MRI). We calculated the volume of the AIS using an easily reproducible methodology (ABC/2). We then identified which patients developed HT after one week of therapy and examined the factors potentially associated with an increased risk of HT. Our study provided useful insights for clinical practice. We observed an increased risk of HT in patients with higher scores on the stroke clinical severity scale (NIHSS), larger infarcts, treatment with mechanical thrombectomy, administration of antiplatelet loading doses and stent placement. Furthermore, we identified a 11-fold increased risk of HT in patients with acute ischaemic lesion volumes on MRI >8.2 ml, and a 6-fold increased risk for patients with NIHSS >4. This study is easily reproducible in clinical practice, as it utilizes readily available clinical and radiological parameters. It highlights how the integration of clinical and radiological data can assist neurologists in navigating grey areas of treatment. In this way, it might be possible to identify patients at risk of haemorrhage, who should be monitored more closely to prevent adverse effects that could lead to the interruption of DAPT, thereby reducing the risk of a new ischemic stroke.
© The Author(s), 2024.
Figures
References
-
- Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke 2021; 52: e364–e467. - PubMed
-
- Kennedy J, Hill MD, Ryckborst KJ, et al. Fast Assessment of Stroke and Transient Ischaemic Attack to Prevent Early Recurrence (FASTER): a randomised controlled pilot trial. Lancet Neurol 2007; 6: 961–969. - PubMed
-
- Wang Y, Wang Y, Zhao X, et al. CHANCE Investigators. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med 2013; 369(1): 11–19. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
