

Performance of Atrial Fibrillation Burden Trends for Stroke Risk Stratification
- PMID: 39445430
- PMCID: PMC11575904
- DOI: 10.1161/CIRCEP.123.012394
Performance of Atrial Fibrillation Burden Trends for Stroke Risk Stratification
Abstract
Background: Atrial fibrillation (AF) is associated with an increased risk of stroke, yet the limitations of conventional monitoring have restricted our understanding of AF burden risk thresholds. Predictive algorithms incorporating continuous AF burden measures may be useful for predicting stroke. This study evaluated the performance of temporal AF burden trends as predictors of stroke from a large cohort with insertable cardiac monitors.
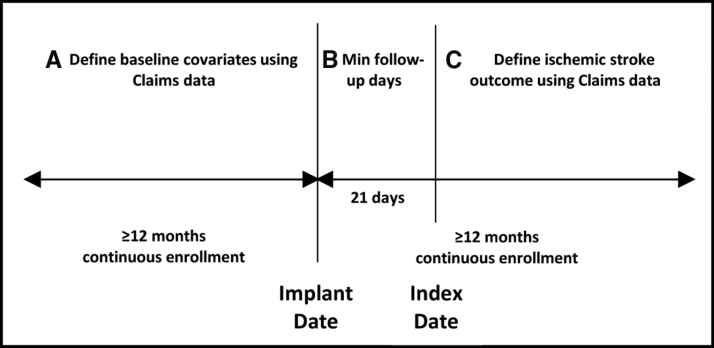
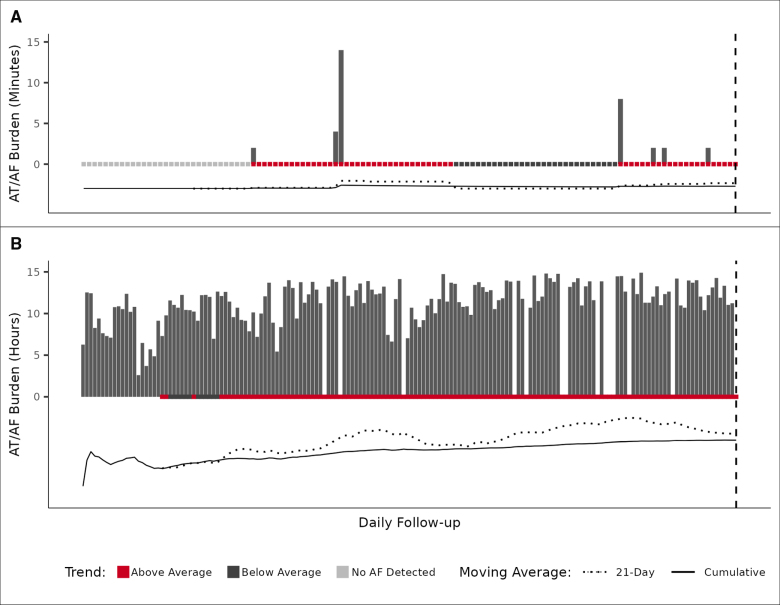
Methods: Using deidentified data from Optum Clinformatics Data Mart (2007-2019) linked with the Medtronic CareLink insertable cardiac monitor database, we identified patients with an insertable cardiac monitor for AF management (n=1197), suspected AF (n=1611), and cryptogenic stroke (n=2205). Daily AF burden was transformed into simple moving averages, and temporal AF burden trends were defined as the comparison of unique simple moving average pairs. Classification trees were used to predict ischemic stroke, and AF burden significance was quantified using bootstrapped mean variable importance.
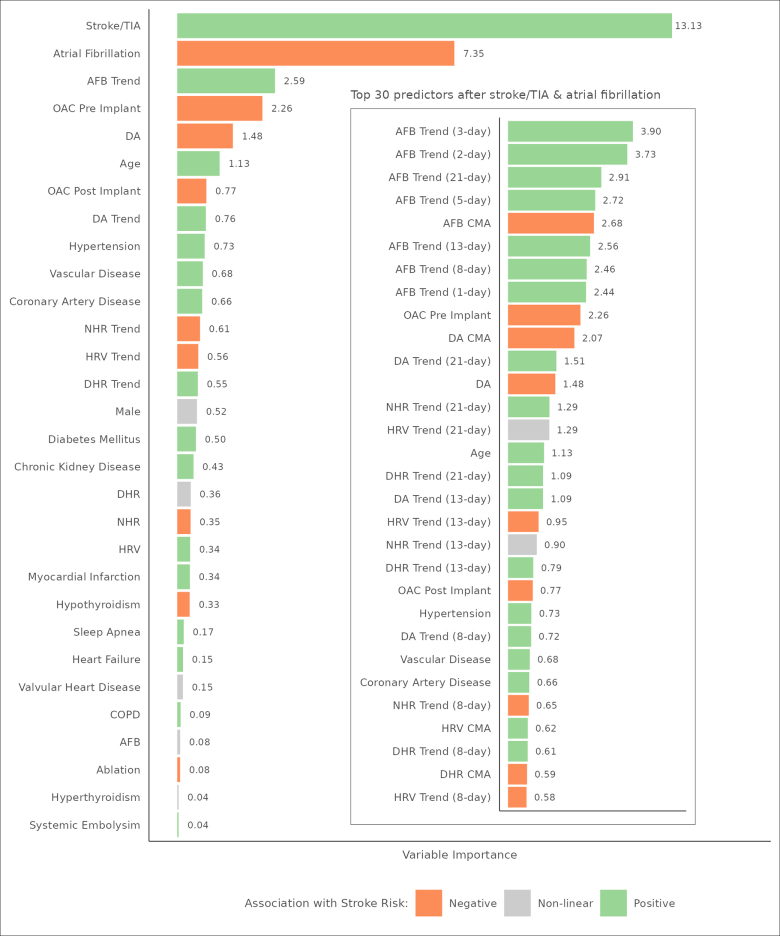
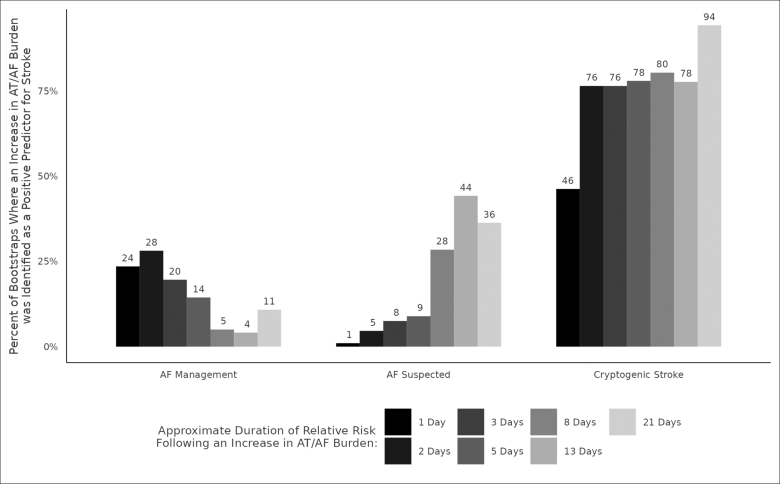
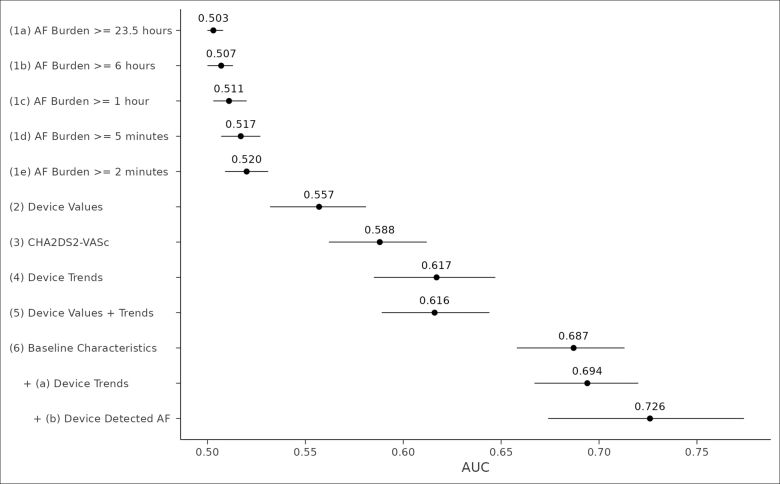
Results: Of 5013 patients (age, 69.2±11.7 years; 50% male; CHA2DS2-VASc, 3.7±1.9) who met inclusion criteria, 869 had an ischemic stroke over 2 409 437 days total follow-up. Prior stroke or transient ischemic attack (variable importance, 13.13) was the number 1 predictor of future stroke followed by no prior diagnosis of AF (7.35) and AF burden trends in follow-up (2.59). Temporal proximity of AF and risk of stroke differed by device indication (simple moving averages: AF management, <8 days and suspected AF and cryptogenic stroke, 8-21 days). Together, baseline characteristics and AF burden trends performed optimally for the area under the receiver operating characteristic curve (0.73), specificity (0.70), and relative risk (5.00).
Conclusions: AF burden trends may provide incremental prognostic value as leading indicators of stroke risk compared with conventional schemes.
Keywords: atrial fibrillation; stroke; thromboembolism; time factors.
Conflict of interest statement
Dr Piccini was supported by grant R01AG074185 from the National Institutes of Aging and grants for clinical research from Abbott, the American Heart Association, the Association for the Advancement of Medical Instrumentation, Bayer, Boston Scientific, iRhythm, and Philips and serves as a consultant to Abbott, Abbvie, Ablacon, Altathera, ARCA Biopharma, Biotronik, Boston Scientific, Bristol Myers Squibb, LivaNova, Medtronic, Milestone, ElectroPhysiology Frontiers, Pfizer, Sanofi, Philips, and Up-to-Date. Dr Hylek serves as a consultant to Bayer, Bristol Myers Squibb, Ionis, Janssen, and Pfizer and received research grants from Abbott, Anthos Therapeutics, and Medtronic and honoraria from Boehringer Ingelheim. Dr Lakkireddy serves as a consultant to Medtronic, Boston Scientific, Abbott, AtriCure, AltaThera, Acutus, and AliveCor. Dr Mittal serves as a consultant to Abbott, Boston Scientific, and Medtronic. Dr Peacock serves as a consultant to Medtronic and Biotronik. Dr Russo serves as a consultant to Abbot, AtriCure, Bayer, Biosense Webster, Boston Scientific, Medtronic, and PaceMate and received grants for clinical research from Boston Scientific, Kestra, Medilynx, and Medtronic and honoraria from Biotronik, Bristol Myers Squibb, Pfizer, Medtronic, and Sanofi. Dr Passman was supported by grant UG3HL165065 from the National Heart, Lung, and Blood Institute, grant 18SFRN34250013 from the American Heart Association, and a grant for clinical research from Abbott; serves as a consultant to Medtronic, Janssen Pharmaceuticals, and Abbott; and receives royalties from Up-To-Date. E.J. Stanelle, Dr Johnson, R. Kanwar, and D. Soderlund are employed by Medtronic. M.T. Hills reports no conflicts.
Figures
References
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, et al. . 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–2104. doi: 10.1161/cir.0000000000000040 - PubMed
-
- Glotzer TV, Hellkamp AS, Zimmerman J, Sweeney MO, Yee R, Marinchak R, Cook J, Paraschos A, Love J, Radoslovich G, et al. ; MOST Investigators. Atrial high rate episodes detected by pacemaker diagnostics predict death and stroke: report of the Atrial Diagnostics Ancillary Study of the MOde Selection Trial (MOST). Circulation. 2003;107:1614–1619. doi: 10.1161/01.CIR.0000057981.70380.45 - PubMed
-
- Healey JS, Connolly SJ, Gold MR, Israel CW, Van Gelder IC, Capucci A, Lau CP, Fain E, Yang S, Bailleul C, et al. . Subclinical atrial fibrillation and the risk of stroke. N Engl J Med. 2012;366:120–129. doi: 10.1056/NEJMoa1105575 - PubMed
-
- Capucci A, Santini M, Padeletti L, Gulizia M, Botto G, Boriani G, Ricci R, Favale S, Zolezzi F, Di Belardino N, et al. ; Italian AT500 Registry Investigators. Monitored atrial fibrillation duration predicts arterial embolic events in patients suffering from bradycardia and atrial fibrillation implanted with antitachycardia pacemakers. J Am Coll Cardiol. 2005;46:1913–1920. doi: 10.1016/j.jacc.2005.07.044 - PubMed
-
- Glotzer TV, Daoud EG, Wyse DG, Singer DE, Ezekowitz MD, Hilker C, Miller C, Qi D, Ziegler PD. The relationship between daily atrial tachyarrhythmia burden from implantable device diagnostics and stroke risk: the TRENDS study. Circ Arrhythm Electrophysiol. 2009;2:474–480. doi: 10.1161/CIRCEP.109.849638 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
