

Effect of Hyperketonemia on Myocardial Function in Patients With Heart Failure and Type 2 Diabetes
- PMID: 39446133
- PMCID: PMC11664025
- DOI: 10.2337/db24-0406
Effect of Hyperketonemia on Myocardial Function in Patients With Heart Failure and Type 2 Diabetes
Abstract
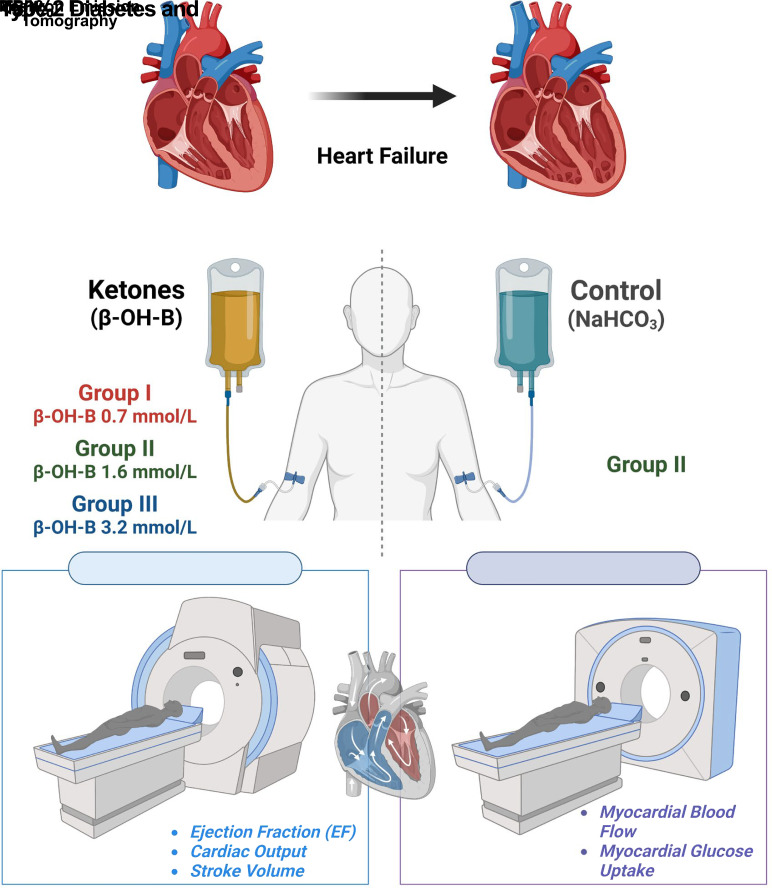
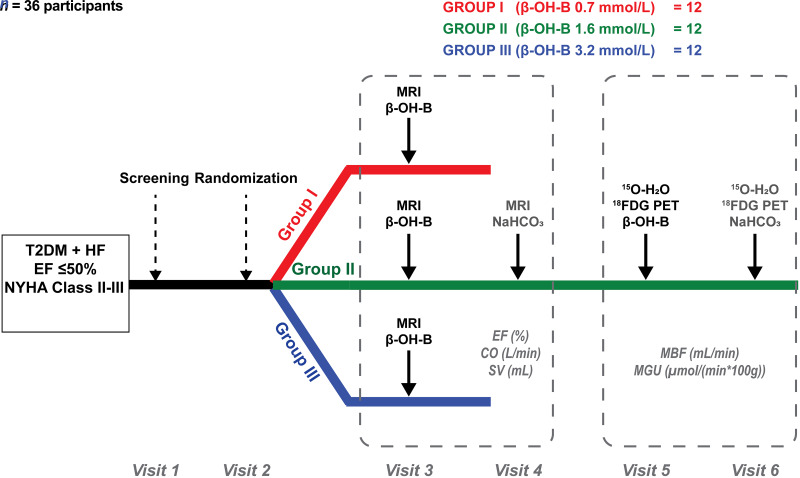
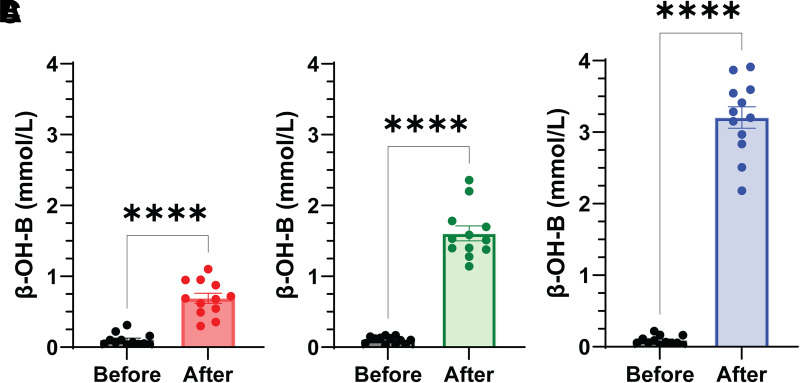
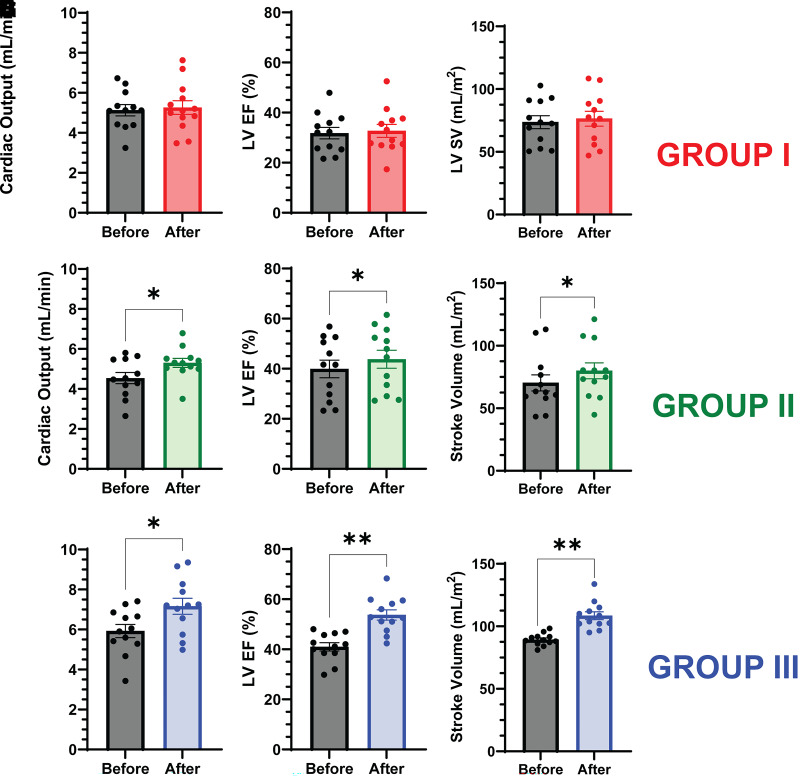
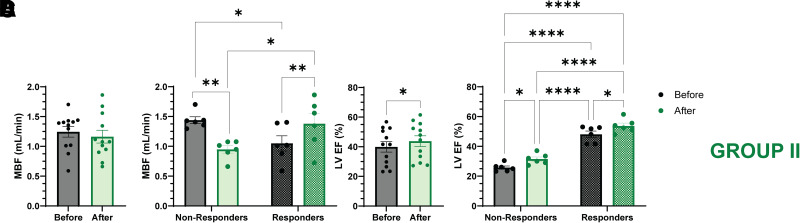
We examined the effect of increased levels of plasma ketones on left ventricular (LV) function, myocardial glucose uptake (MGU), and myocardial blood flow (MBF) in patients with type 2 diabetes (T2DM) with heart failure. Three groups of patients with T2DM (n = 12 per group) with an LV ejection fraction (EF) ≤50% received incremental infusions of β-hydroxybutyrate (β-OH-B) for 3-6 h to increase the plasma β-OH-B concentration throughout the physiologic (groups I and II) and pharmacologic (group III) range. Cardiac MRI was performed at baseline and after each β-OH-B infusion to provide measures of cardiac function. On a separate day, group II also received a sodium bicarbonate (NaHCO3) infusion, thus serving as their own control for time, volume, and pH. Additionally, group II underwent positron emission tomography study with 18F-fluoro-2-deoxyglucose to examine effect of hyperketonemia on MGU. Groups I, II, and III achieved plasma β-OH-B levels (mean ± SEM) of 0.7 ± 0.3, 1.6 ± 0.2, 3.2 ± 0.2 mmol/L, respectively. Cardiac output (CO), LVEF, and stroke volume (SV) increased significantly during β-OH-B infusion in groups II (CO, from 4.54 to 5.30; EF, 39.9 to 43.8; SV, 70.3 to 80.0) and III (CO, from 5.93 to 7.16; EF, 41.1 to 47.5; SV, 89.0 to 108.4), and did not change with NaHCO3 infusion in group II. The increase in LVEF was greatest in group III (P < 0.001 vs. group II). MGU and MBF were not altered by β-OH-B. In patients with T2DM and LVEF ≤50%, increased plasma β-OH-B level significantly increased LV function dose dependently. Because MGU did not change, the myocardial benefit of β-OH-B resulted from providing an additional fuel for the heart without inhibiting MGU.
© 2024 by the American Diabetes Association.
Conflict of interest statement
Figures
References
-
- Benjamin EJ, Virani SS, Callaway CW, et al.; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation 2018;137:e67–e492 - PubMed
-
- Nichols GA, Gullion CM, Koro CE, Ephross SA, Brown JB.. The incidence of congestive heart failure in type 2 diabetes: an update. Diabetes Care 2004;27:1879–1884 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
