

The Bidirectional Effects of Periodontal Disease and Oral Dysbiosis on Gut Inflammation in Inflammatory Bowel Disease
- PMID: 39447062
- PMCID: PMC12041420
- DOI: 10.1093/ecco-jcc/jjae162
The Bidirectional Effects of Periodontal Disease and Oral Dysbiosis on Gut Inflammation in Inflammatory Bowel Disease
Abstract
Background and aims: Inflammatory bowel disease (IBD) flares can lead to excessive morbidity and mortality. This study aimed to determine whether oral dysbiosis/periodontal disease (PD) is common in IBD and is associated with disease activity in IBD.
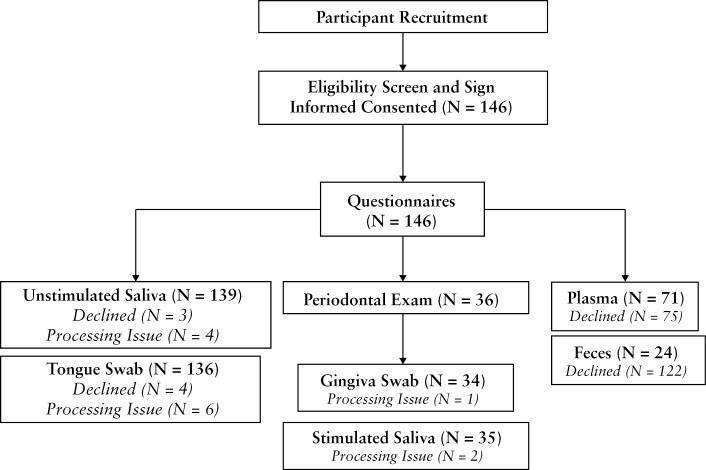
Methods: This single-center, prospective, cross-sectional, proof-of-concept, and observational study assessed the frequency of periodontal inflammatory disease and interrogated oral and stool microbiota using 16S rRNA gene amplicon sequencing of active-IBD (aIBD), inactive-IBD (iIBD), and healthy controls (HC). Questionnaires assessed diet, alcohol usage, oral hygiene behavior, and disease activity. A subset of participants underwent comprehensive dental examinations to evaluate PD.
Results: Periodontal disease was severer in aIBD subjects than in HC, as aIBD had poorer quality diets (lower Mediterranean diet scores) than iIBD and HC. Significant differences in microbial community structure were observed in unstimulated saliva, stimulated saliva, gingiva, and stool samples, primarily between aIBD and HC. Saliva from aIBD had higher relative abundances of putative oral pathobionts from the genera Streptococcus, Granulicatella, Rothia, and Actinomyces relative to HC, despite similar oral hygiene behaviors between groups.
Conclusions: Our study suggests that patients with aIBD have severer periodontal disorders and higher relative abundances of putative 'pro-inflammatory' microbiota in their oral cavity, despite normal oral hygiene behaviors. Our data are consistent with the potential presence of an oral-gut inflammatory axis that could trigger IBD flare-ups in at-risk patients. Routine dental health assessments in all IBD patients should be encouraged as part of the health maintenance of IBD and as a potential strategy to decrease the risk of IBD flares.
Keywords: dysbiosis; inflammatory bowel disease; microbiota; oral hygiene; periodontal disease.
© The Author(s) 2024. Published by Oxford University Press on behalf of European Crohn’s and Colitis Organisation. All rights reserved. For commercial re-use, please contact reprints@oup.com for reprints and translation rights for reprints. All other permissions can be obtained through our RightsLink service via the Permissions link on the article page on our site—for further information please contact journals.permissions@oup.com.
Conflict of interest statement
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as potential conflicts of interest. Guarantor of the article: Ali Keshavarzian, MD.
Figures



References
-
- Brakenhoff LK, van der Heijde DM, Hommes DW, Huizinga TW, Fidder HH.. The joint-gut axis in inflammatory bowel diseases. J Crohns Colitis 2010;4:257–68. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
