

Pharmacotherapy for behavioural manifestations in frontotemporal dementia: An expert consensus from the European Reference Network for Rare Neurological Diseases (ERN-RND)
- PMID: 39447217
- PMCID: PMC11555005
- DOI: 10.1111/ene.16446
Pharmacotherapy for behavioural manifestations in frontotemporal dementia: An expert consensus from the European Reference Network for Rare Neurological Diseases (ERN-RND)
Erratum in
-
Correction to "Pharmacotherapy for behavioural manifestations in frontotemporal dementia: An expert consensus from the European Reference Network for Rare Neurological Diseases (ERN-RND)".Eur J Neurol. 2025 Mar;32(3):e70108. doi: 10.1111/ene.70108. Eur J Neurol. 2025. PMID: 40047121 Free PMC article. No abstract available.
Abstract
Background and purpose: Frontotemporal dementia (FTD) is a neurodegenerative disorder characterized by pervasive personality and behavioural disturbances with severe impact on patients and caregivers. In current clinical practice, treatment is based on nonpharmacological and pharmacological approaches. Unfortunately, trial-based evidence supporting symptomatic pharmacological treatment for the behavioural disturbances in FTD is scarce despite the significant burden this poses on the patients and caregivers.
Method: The study examined drug management decisions for several behavioural disturbances in patients with FTD by 21 experts across European expert centres affiliated with the European Reference Network for Rare Neurological Diseases (ERN-RND).
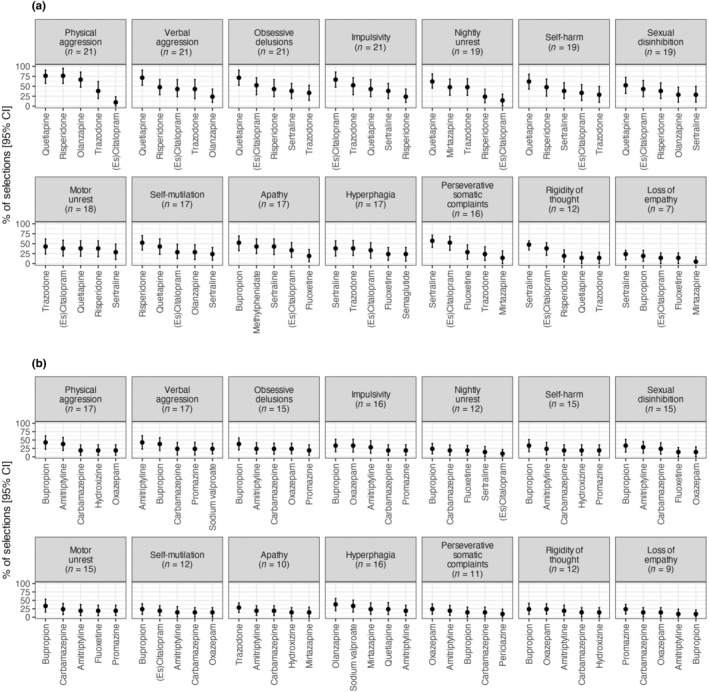
Results: The study revealed the highest consensus on drug treatments for physical and verbal aggression, impulsivity and obsessive delusions. Antipsychotics (primarily quetiapine) were recommended for behaviours posing safety risks to both patients and caregivers (aggression, self-injury and self-harm) and nightly unrest. Selective serotonin reuptake inhibitors were recommended for perseverative somatic complaints, rigidity of thought, hyperphagia, loss of empathy and for impulsivity. Trazodone was specifically recommended for motor unrest, mirtazapine for nightly unrest, and bupropion and methylphenidate for apathy. Additionally, bupropion was strongly advised against in 10 out of the 14 behavioural symptoms, emphasizing a clear recommendation against its use in the majority of cases.
Conclusions: The survey data can provide expert guidance that is helpful for healthcare professionals involved in the treatment of behavioural symptoms. Additionally, they offer insights that may inform prioritization and design of therapeutic studies, particularly for existing drugs targeting behavioural disturbances in FTD.
Keywords: drug therapy; expert testimony; frontotemporal dementia; neurobehavioural manifestations; neurodegenerative diseases.
© 2024 The Author(s). European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
Johannes Levin reports receiving speaker fees from Bayer Vital, Biogen, EISAI, TEVA, Zambon, Merck, and Roche, as well as consulting fees from Axon Neuroscience, EISAI, and Biogen. He has also received author fees from Thieme Medical Publishers and W. Kohlhammer GmbH Medical Publishers. Johannes Levin is the inventor of a patent titled "Oral Phenylbutyrate for Treatment of Human 4‐Repeat Tauopathies" (EP 23 156 122.6) filed by LMU Munich. Additionally, he serves as the Chief Medical Officer for MODAG GmbH, is a beneficiary of MODAG GmbH's phantom share program, and is the inventor of a patent titled "Pharmaceutical Composition and Methods of Use" (EP 22 159 408.8) filed by MODAG GmbH. All of these activities are unrelated to the work submitted. Jonathan Rohrer has provided consultancy services or served on advisory boards for Novartis, Wave Life Sciences, Prevail, Alector, Aviado Bio, Takeda, Arkuda Therapeutics, and Denali Therapeutics.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
