

Interferon-gamma driven elevation of CXCL9: a new sepsis endotype independently associated with mortality
- PMID: 39447386
- PMCID: PMC11539129
- DOI: 10.1016/j.ebiom.2024.105414
Interferon-gamma driven elevation of CXCL9: a new sepsis endotype independently associated with mortality
Abstract
Background: Endotype classification becomes the cornerstone of understanding sepsis pathogenesis. Macrophage activation-like syndrome (MALS) and immunoparalysis are the best recognized major endotypes, so far. Interferon-gamma (IFNγ) action on tissue macrophages stimulates the release of the cytotoxic chemokine CXCL9. It was investigated if this mechanism may be an independent sepsis endotype.
Methods: In this cohort study, 14 patient cohorts from Greece, Germany and Italy were studied. The cohorts were 2:1 randomly split into discovery and validation sets. Sepsis was defined by the Sepsis-3 definitions and blood was sampled the first 24 h from meeting the Sepsis-3 definitions. Concentrations of IFNγ, CXCL9, IP-10 (IFNγ induced protein-10), soluble CD163 and ferritin were measured. The endotype of IFNγ-driven sepsis (IDS) was defined in the discovery set as the combination of a) blood IFNγ above a specified cut-off associated with the minimal risk for immunoparalysis (defined as ≥8000 HLA-DR receptors on CD45/CD14-monoytes); and b) increase of CXCL9. Results were compared to the validation set.
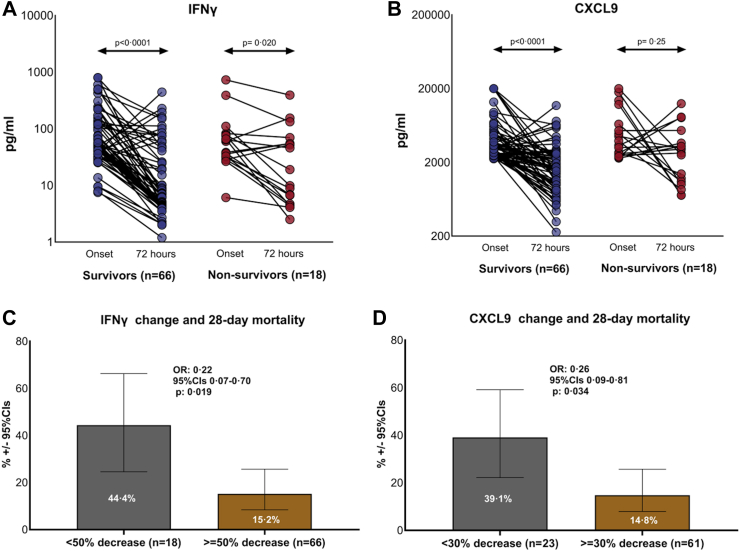
Findings: 5503 patients were studied; 3670 in the discovery set and 1833 in the validation set. IDS was defined as IFNγ more than 3 pg/ml and CXCL9 more than 2200 pg/ml. The frequency of IDS in the discovery set was 19.9% (732 patients; 95% confidence intervals-CIs 18.7-21.3%) and in the validation set 20.0% (366 patients; 95% CIs 18.2-21.9%). Soluble CD163, a marker of macrophage activation, was greater in IDS and IDS had features distinct from MALS. The mortality in IDS patients was 43.0% (315 patients; 95% CIs 39.5-46.6%) in the discovery set and 40.4% in the validation set (148 patients; 95% CIs 35.5-45.5%) (p = 0.44 compared to patients of the discovery set). IDS was an independent risk factor for death in the presence of other endotypes, severity scores and organ dysfunctions of the multivariate model [hazard ratio 1.71 (95% CIs 1.45-2.01) in the discovery set and 1.70 (95% CIs 1.34-2.16) in the validation set]. Decreases of IFNγ and CXCL9 blood levels within the first 72 h were associated with better outcome.
Interpretation: IDS is a new sepsis endotype independently associated with unfavorable outcome.
Funding: Hellenic Institute for the Study of Sepsis; Horizon 2020 project ImmunoSep; Swedish Orphan BioVitrum AB (publ) and German Federal Ministry of Education and Research.
Keywords: CXCL9; Interferon-gamma; Macrophages; Outcome; Sepsis.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests EJG-B reports honoraria and consultation fees from Abbott Products Operations, bioMérieux, Brahms GmbH, GSK and Sobi (granted to the National and Kapodistrian University of Athens); independent educational grants from AbbVie, InCyte, Novartis and UCB (granted to the National and Kapodistrian University of Athens) and from Abbott Products Operations, bioMérieux Inc, Johnson & Johnson, MSD, and Swedish Orphan Biovitrum AB (granted to the Hellenic Institute for the Study of Sepsis); and funding from the Horizon 2020 European Grants ImmunoSep and RISCinCOVID and the Horizon Health grants EPIC-CROWN-2, POINT and Homi-Lung (granted to the Hellenic Institute for the Study of Sepsis). MA reports Honoraria for Board Participation from Shionogi, Pfizer and Menarini and unrestricted research grants from GE and Fisher and Paykel. AJR is a full-time employee of Sobi. The authors FB and DT-R were supported by the German Federal Ministry of Education and Research (BMBF; grant number 01KU2209) within the ERA PerMed project iRECORDS. MK is inventor of a patent covering a method for quantification of C-terminal peptides of AAT (applicant: Jena University Hospital) (JUH); EP4224163A1; status: application), and the inventor of other patents covering C-terminal AAT peptides in inflammation (applicant: Jena University Hospital (JUH): Method for determining the origin of an infection (EP3239712B1 [granted]) and Diagnosis of Sepsis and Systemic Inflammatory Response Syndrome (EP2592421B1, EP2780719B1, CN104204808B, US10712350B2, JP6308946B2 [all granted]). MB is cofounder of SmartDyeLivery GmbH, Jena, and declares receipt of independent educational grants from B.R.A.H.M.S/Thermofisher, Swedish Orphan Biovitrum AB; and funding from the Horizon 2020 European Grants ImmunoSep and by the German Federal Ministry of Education and Research (BMBF; grant number 01KU2209) within the ERA PerMed project iRECORDS and the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) Project Number 316213987—SFB 1278 “PolyTarget” (Project C06). The other authors do not declare any conflict of interest.
Figures




References
-
- Pan M., wei X., Xiang X., Lu Y., Zhou Q., Yang W. Targeting CXCL9/10/11–CXCR3 axis: an important component of tumor-promoting and antitumor immunity. Clin Transl Oncol. 2023;25:2306–2320. - PubMed
-
- House I.G., Derrick E.B., Sek K., et al. CRISP-Cas9 secreening indentifies an IRF-SOCS-1-mediated negative feedback loop that limits CXCL9 expression and anitumor activity. Cell Rep. 2023;42 - PubMed
-
- Ibadullaeva N., Khikmatullaeva A., Mirzaev U., et al. Identification of CXCL9 chemokine as apotenital biomarker for assessing clinical severity in COVID-19 patients. J Infect Dev Cntries. 2024;18:672–678. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
