

Temporal trends in concordance between ICD-coded and cardiac biomarker-classified hospitalisation rates for acute coronary syndromes: a linked hospital and biomarker data study
- PMID: 39448082
- PMCID: PMC11499754
- DOI: 10.1136/openhrt-2024-002995
Temporal trends in concordance between ICD-coded and cardiac biomarker-classified hospitalisation rates for acute coronary syndromes: a linked hospital and biomarker data study
Abstract
Background: Since 2000, the definition of myocardial infarction (MI) has evolved with reliance on cardiac troponin (cTn) tests. The implications of this change on trends of acute coronary syndrome (ACS) subtypes obtained from routinely collected hospital morbidity data are unclear. Using person-linked hospitalisation data, we compared International Classification of Diseases (ICD)-coded data with biomarker-classified admission rates for ST-segment elevation MI (STEMI), non-STEMI (NSTEMI) and unstable angina (UA) in Western Australia (WA).
Methods: We used linked hospitalisation data from all WA tertiary hospitals to identify patients with a principal diagnosis of STEMI, NSTEMI or UA between 2002 and 2016. Linked biomarker results were classified as 'diagnostic' for MI according to established criteria. We calculated age-standardised and sex-standardised rates (ASSRs) for ICD-coded versus biomarker-classified admissions by ACS subtypes and estimated annual change in admissions using Poisson regression adjusting for age and sex.
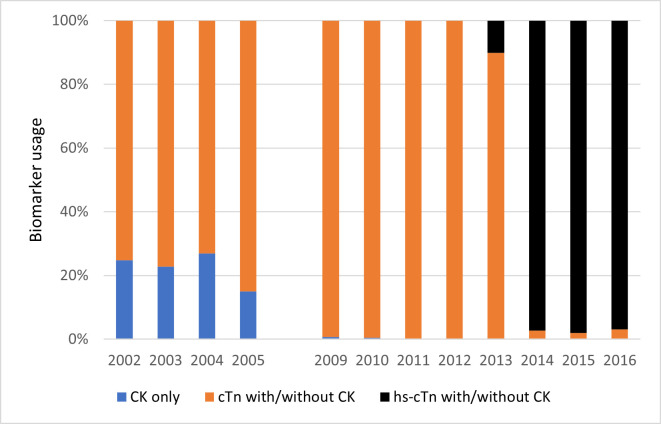
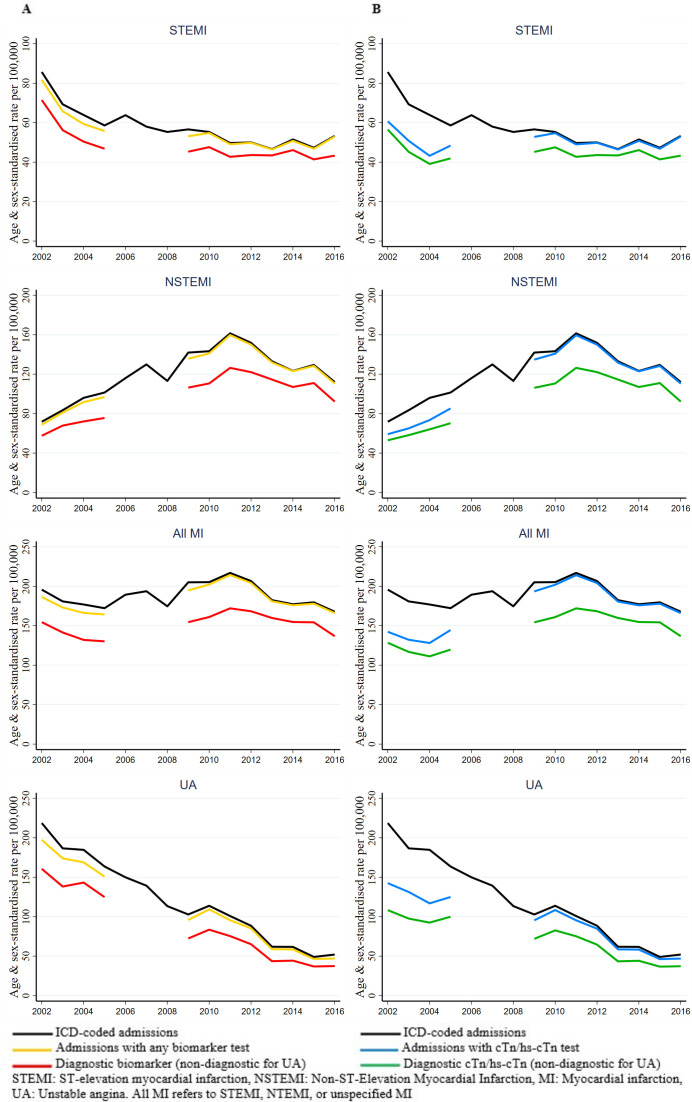
Results: There were 37 272 ACS admissions in 30 683 patients (64.2% male), and 96% of cases had linked biomarker data, predominantly conventional cTn at the start and high-sensitive cTn from late 2013. Despite lower ASSRs, trends in MI classified with a diagnostic biomarker were concordant with ICD-coded admissions rates for both STEMI and NSTEMI. Between 2002 and 2010, STEMI rates declined by 4.1% (95% CI 5.0%, 3.1%) and 3.4% (95% CI 4.6%, 2.3%) in ICD-coded and biomarker-classified admissions, respectively, and both plateaued thereafter. For NSTEMI between 2002 and 2010, the ICD-coded and biomarker-classified rates increased 8.0% per year (95% CI 7.2%, 8.9%) and 8.0% (95% CI 7.0%, 9.0%), respectively, and both subsequently declined. For UA, both ICD-coded and biomarker-classified UA admission rates declined in a steady and concordant manner between 2002 and 2016.
Conclusions: The present study supports the validity of using administrative data to monitor population trends in ACS subtypes as they appear to generally reflect the redefinition of MI in the troponin era.
Keywords: Acute Coronary Syndrome; Biomarkers; EPIDEMIOLOGY.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Nationwide trends in acute coronary syndrome by subtype in New Zealand 2006-2016.Heart. 2020 Feb;106(3):221-227. doi: 10.1136/heartjnl-2019-315655. Epub 2019 Oct 31. Heart. 2020. PMID: 31672778
-
Epidemiology and risk factors of patients with types of acute coronary syndrome presenting to a tertiary care hospital in Sri Lanka.BMC Cardiovasc Disord. 2019 Oct 21;19(1):229. doi: 10.1186/s12872-019-1217-x. BMC Cardiovasc Disord. 2019. PMID: 31638908 Free PMC article.
-
Validation of ICD-10-AM Coding for Myocardial Infarction Subtype in Hospitalisation Data.Heart Lung Circ. 2022 Jun;31(6):849-858. doi: 10.1016/j.hlc.2021.11.014. Epub 2022 Jan 20. Heart Lung Circ. 2022. PMID: 35065895
-
Contemporary NSTEMI management: the role of the hospitalist.Hosp Pract (1995). 2020 Feb;48(1):1-11. doi: 10.1080/21548331.2020.1701329. Epub 2020 Feb 20. Hosp Pract (1995). 2020. PMID: 31815570 Review.
-
Diagnosis and Treatment of Acute Coronary Syndromes: A Review.JAMA. 2022 Feb 15;327(7):662-675. doi: 10.1001/jama.2022.0358. JAMA. 2022. PMID: 35166796 Review.
References
-
- Rogers WJ, Frederick PD, Stoehr E, et al. Trends in presenting characteristics and hospital mortality among patients with ST elevation and non-ST elevation myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am Heart J. 2008;156:1026–34. doi: 10.1016/j.ahj.2008.07.030. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources