

Surgical conditions in experimental laparoscopy: effects of pressure, neuromuscular blockade, and pre-stretching on workspace volume
- PMID: 39448406
- PMCID: PMC11614944
- DOI: 10.1007/s00464-024-11338-0
Surgical conditions in experimental laparoscopy: effects of pressure, neuromuscular blockade, and pre-stretching on workspace volume
Abstract
Background: Establishing a pneumoperitoneum for laparoscopy is common surgical practice, with the goal to create an optimal surgical workspace within the abdominal cavity while minimizing insufflation pressure. Individualized strategies, based on neuromuscular blockade (NMB), pre-stretching routines, and personalized intra-abdominal pressure (IAP) to enhance surgical conditions are strategies to improve surgical workspace. However, the specific impact of each factor remains uncertain. This study explores the effects and side-effects of modifying intra-abdominal volume (IAV) through moderate and complete NMB in a porcine laparoscopy model.
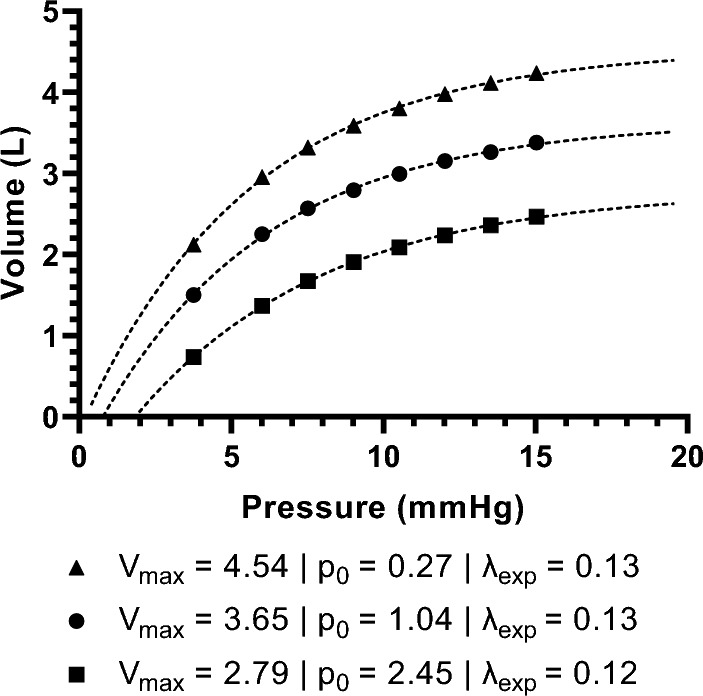
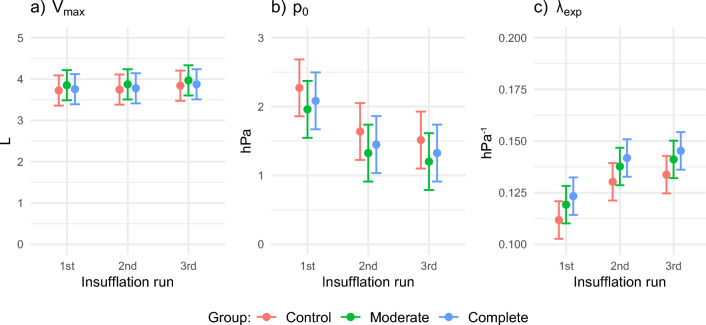
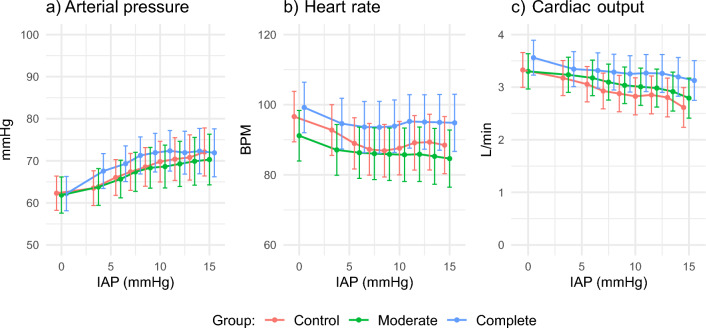
Methods: Thirty female Landrace pigs were randomly assigned to groups with complete NMB, regular NMB and a control group. Varying IAP levels were applied, and IAV was measured using CT scans. The study evaluated the maximum attainable IAV (Vmax), the pressure at which the cavity opens (p0), and the ease of expansion (λexp). Cardiorespiratory parameters, including peak inspiratory pressure (PIP), mean arterial pressure (MAP), heart rate (HR), and cardiac output (CO), were continuously recorded to evaluate side-effects.
Results: There were no significant weight differences between NMB groups (median 21.1 kg). Observed volumes ranged from 0 to 4.7 L, with a mean Vmax of 3.82 L, mean p0 of 1.23 mmHg, and mean λexp of 0.13 hPa-1. NMB depth did not significantly affect these parameters. HR was significantly increased in the complete NMB group, while PIP, MAP, and CO remained unaffected. Repeated insufflation positively impacted Vmax; ease of opening; and expanding the cavity.
Conclusion: In this porcine model, the depth of NMB does not alter abdominal mechanics or increase the surgical workspace. Cardiorespiratory changes are more related to insufflation pressure and frequency rather than NMB depth. Future studies should compensate for the positive effect of repeated insufflation on abdominal mechanics and surgical conditions.
Keywords: Insufflation; Neuromuscular blockade; Surgical workspace.
© 2024. The Author(s).
Conflict of interest statement
Disclosures: Erasmus MC received partial funding from Health ~ Holland (LSHM17063) and Merck Sharp & Dohme Corp (ISS57163). Erasmus MC holds patents on improved insufflation devices, with Willem van Weteringen, John Vlot, and Frank Sterke as inventors. John Vlot received an insufflation device from Karl Storz SE & Co. KG. Willem van Weteringen and Frank Sterke are partially employed by an Erasmus MC spin-off developing an enhanced insufflator. Philip van der Zee, Joost van Rosmalen, and René Wijnen have no conflicts of interest.
Figures
References
-
- Neugebauer EA, Sauerland S, Fingerhut A, Millat B, Buess G (2006) EAES guidelines for endoscopic surgery. Springer, Berlin
-
- Díaz-Cambronero O, Mazzinari G, Flor Lorente B, García Gregorio N, Robles-Hernandez D, Olmedilla Arnal LE, Martin de Pablos A, Schultz MJ, Errando CL, Argente Navarro MP (2020) Effect of an individualized versus standard pneumoperitoneum pressure strategy on postoperative recovery: a randomized clinical trial in laparoscopic colorectal surgery. Br J Surg 107:1605–1614. 10.1002/bjs.11736 - DOI - PubMed
-
- Fuchs-Buder T, De Robertis E, Brunaud L (2018) Neuromuscular block in laparoscopic surgery. Minerva Anestesiol 84:509–514. 10.23736/S0375-9393.17.12330-8 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
