

A refined TTC assay precisely detects cardiac injury and cellular viability in the infarcted mouse heart
- PMID: 39448689
- PMCID: PMC11502796
- DOI: 10.1038/s41598-024-76414-w
A refined TTC assay precisely detects cardiac injury and cellular viability in the infarcted mouse heart
Abstract
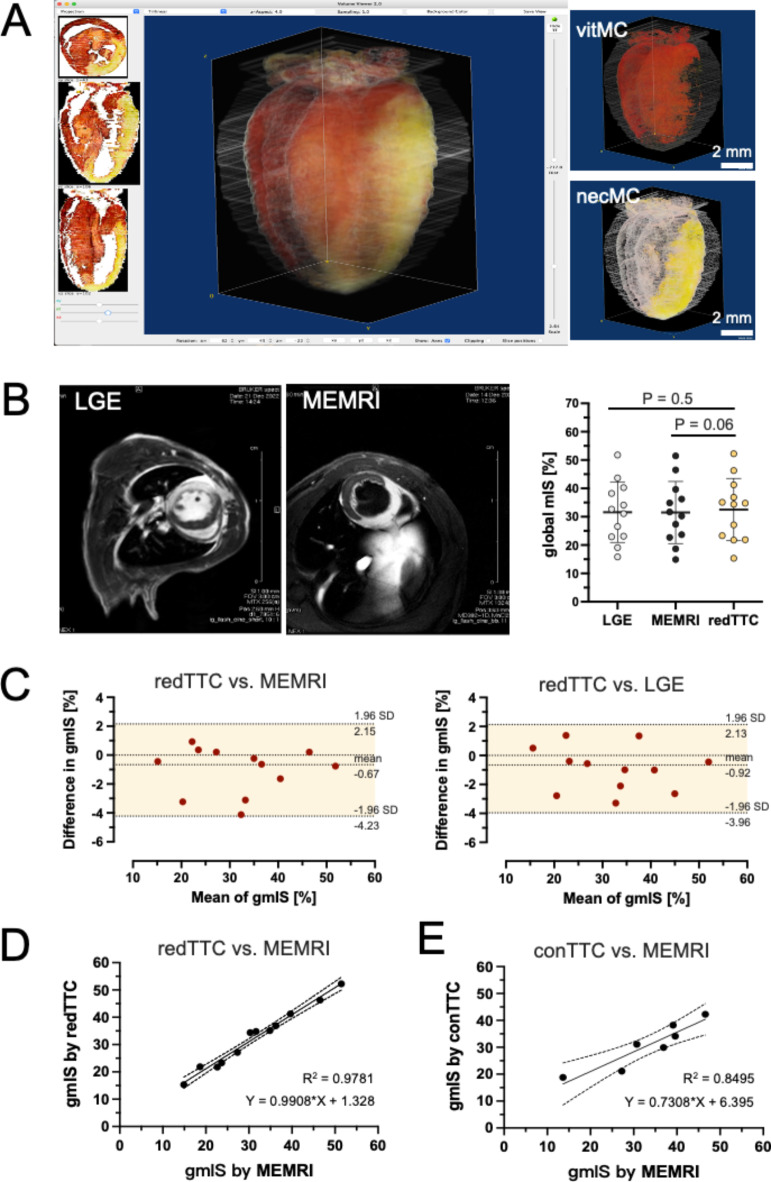
Histological analysis with 2,3,5-triphenyltetrazolium chloride (TTC) staining is the most frequently used tool to detect myocardial ischemia/reperfusion injury. However, its practicality is often challenged by poor image quality in gross histology, leading to an equivocal infarct-boundary delineation and potentially compromised measurement accuracy. Here, we introduce several crucial refinements in staining protocol and sample processing, which enable TTC images to be analyzed with light microscopy. The refined protocol involves a two-step TTC staining process (perfusion and immersion) and subsequent Zamboni fixation to differentiate myocardial viability and necrosis, and use of Coomassie brilliant blue to label area-at-risk. After the duo-staining steps were completed, the heart sample was embedded and sliced transversally by a cryostat into a series of thin sections (50 µm) for microscopic analysis. The refined TTC (redTTC) assay yielded remarkably high-quality images with striking color intensity and sharply defined boundaries, permitting unambiguous and reliable delineation of the infarct and area-at-risk. In the same animals, the redTTC assay showed good agreement with the in-vivo gold standard measurements (LGE and MEMRI). Meanwhile, redTTC imaging allows tracking of viable cardiomyocytes at cellular resolution, and with this enhanced capability, we convincingly demonstrated the pro-survival action of stem cells based-therapy. Therefore, the redTTC assay represents a significant technical advance that permits precise detection of the true extent of cardiac injury and cardiomyocyte viability. This approach is cost-effective and may be adapted for use in diverse applications, making it highly appealing to many laboratories performing ischemia/reperfusion injury experiments.
Keywords: Area-at-risk (AAR); CBB; Cardioprotection; Myocardial infarct size (mIS); Myocardial infarction; redTTC.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Bolli, R. et al. Myocardial protection at a crossroads: The need for translation into clinical therapy. Circ. Res.95, 125–134 (2004). - PubMed
-
- Rich, P. R., Mischis, L. A., Purton, S. & Wiskich, J. T. The sites of interaction of triphenyltetrazolium chloride with mitochondrial respiratory chains. FEMS Microbiol. Lett.202, 181–187 (2001). - PubMed
-
- Birnbaum, Y., Hale, S. L. & Kloner, R. A. Differences in reperfusion length following 30 minutes of ischemia in the rabbit influence infarct size, as measured by triphenyltetrazolium chloride staining. J. Mol. Cell. Cardiol.29, 657–666 (1997). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
