

BCL11A intellectual developmental disorder: defining the clinical spectrum and genotype-phenotype correlations
- PMID: 39448799
- PMCID: PMC11893779
- DOI: 10.1038/s41431-024-01701-z
BCL11A intellectual developmental disorder: defining the clinical spectrum and genotype-phenotype correlations
Abstract
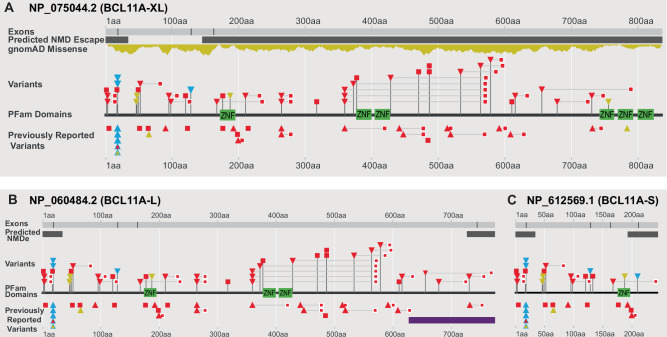
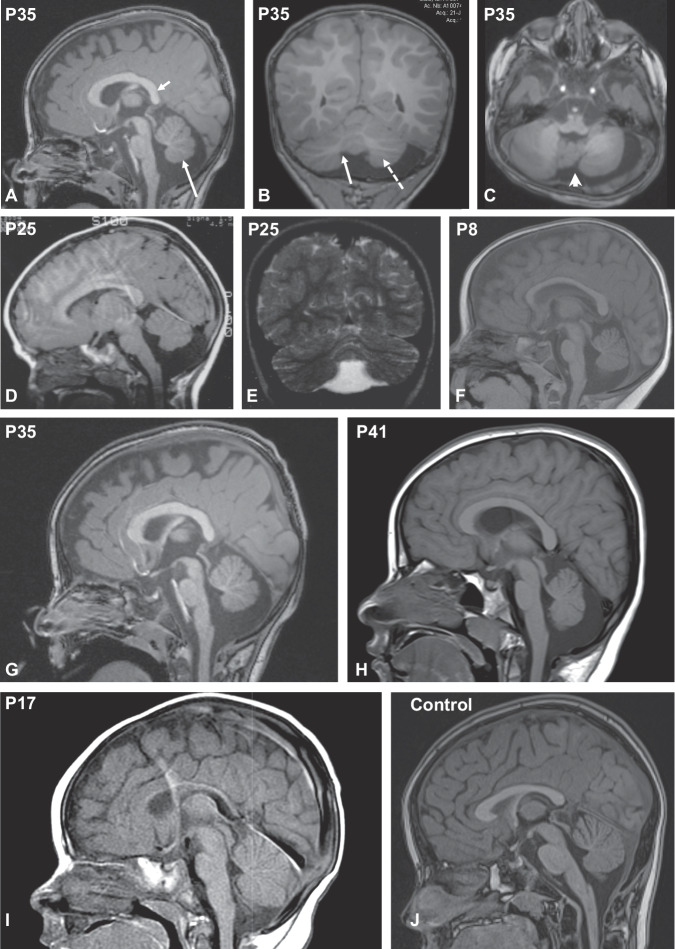
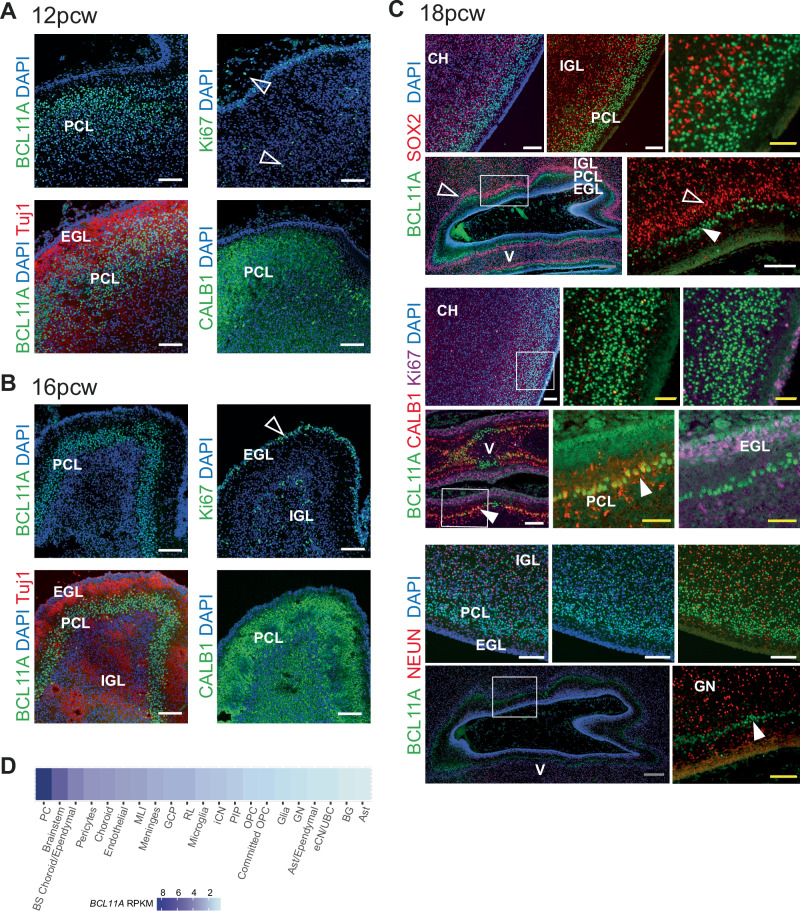
An increasing number of individuals with intellectual developmental disorder (IDD) and heterozygous variants in BCL11A are identified, yet our knowledge of manifestations and mutational spectrum is lacking. To address this, we performed detailed analysis of 42 individuals with BCL11A-related IDD (BCL11A-IDD, a.k.a. Dias-Logan syndrome) ascertained through an international collaborative network, and reviewed 35 additional previously reported patients. Analysis of 77 affected individuals identified 60 unique disease-causing variants (30 frameshift, 7 missense, 6 splice-site, 17 stop-gain) and 8 unique BCL11A microdeletions. We define the most prevalent features of BCL11A-IDD: IDD, postnatal-onset microcephaly, hypotonia, behavioral abnormalities, autism spectrum disorder, and persistence of fetal hemoglobin (HbF), and identify autonomic dysregulation as new feature. BCL11A-IDD is distinguished from 2p16 microdeletion syndrome, which has a higher incidence of congenital anomalies. Our results underscore BCL11A as an important transcription factor in human hindbrain development, identifying a previously underrecognized phenotype of a small brainstem with a reduced pons/medulla ratio. Genotype-phenotype correlation revealed an isoform-dependent trend in severity of truncating variants: those affecting all isoforms are associated with higher frequency of hypotonia, and those affecting the long (BCL11A-L) and extra-long (-XL) isoforms, sparing the short (-S), are associated with higher frequency of postnatal microcephaly. With the largest international cohort to date, this study highlights persistence of fetal hemoglobin as a consistent biomarker and hindbrain abnormalities as a common feature. It contributes significantly to our understanding of BCL11A-IDD through an extensive unbiased multi-center assessment, providing valuable insights for diagnosis, management and counselling, and into BCL11A's role in brain development.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: RP, MD and IMW are employees of GeneDx, Inc. a fee-for-service testing laboratory. MJB is Chair of the Scientific Advisory Board of GeneDx. The other authors declare no competing interests. Ethical approval: The case series was recorded under clinical audit #12785 at Guy’s & St. Thomas’ NHS Foundation Trust. Written informed consent from patient or legal guardian were obtained from the research studies under protocols approved by the following research ethics committees / institutional review boards: Deciphering Developmental Disorders Study: Cambridge South REC reference 10/H0305/83, and Republic of Ireland REC GEN/284/12; The 100,000 Genomes Project: Cambridge South REC 14/EE/1112. The BUILD Study: London - Camden & Kings Cross REC 17/LO/0981. Seattle Children’s Hospital IRB study #13291. IRB Commissie Mensgebonden Onderzoek Regio Arnhem-Nijmegen, CMO approval #NL36191.091.11. Translational Genomics Research Institute: WCG IRB Protocol #20120789. Ethical review board of Friedrich-Alexander-University, Erlangen-Nürnberg, Germany. Rambam Medical Center IRB #0038-14-RBM; Ethics committee of Federico II University Hospital, protocol number 48/16; Johns Hopkins Medicine IRB protocol IRB00214093. For clinically ascertained individuals where IRB waiver is required (Alberta Children’s Hospital REB, Comissão de Ética Hospital Pediátrico Centro Hospitalar Universidade de Coimbra), waiver was confirmed; informed patient/guardian consent was given for publication of de-identified data, including photographs where applicable, and the appropriate institutional forms have been archived in accordance with the principles stated in the Declaration of Helsinki. Only photographs where consent forms are consistent with Springer Nature editorial policies are included in the manuscript.
Figures

References
-
- Peron A, Bradbury K, Viskochil DH, Dias C. BCL11A-Related Intellectual Disability. In: Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Mirzaa G, et al., editors. GeneReviews(®). Seattle (WA): University of Washington, Seattle; 2019. - PubMed
-
- Wiegreffe C, Simon R, Peschkes K, Kling C, Strehle M, Cheng J, et al. Bcl11a (Ctip1) Controls Migration of Cortical Projection Neurons through Regulation of <em>Sema3c</em>. Neuron 2015;87:311–25. - PubMed
