

Hypertension and diabetes control: faith-based centres offer a promise for expanding screening services and linkage to care in Ghana
- PMID: 39448912
- PMCID: PMC11520115
- DOI: 10.1186/s12875-024-02620-0
Hypertension and diabetes control: faith-based centres offer a promise for expanding screening services and linkage to care in Ghana
Abstract
Background: Hypertension and type 2 diabetes mellitus (T2DM) are important contributors to noncommunicable disease related morbidity and mortality. Health systems could benefit from exploring the use of Faith-Based Centres (FBC) to screen and link suspected cases for further care in order to help achieve Sustainable Development Goal (SDG) 3. The study investigated the role of faith-based screening for T2DM and hypertension and the linkage of cases to the healthcare system and examined the care cascade in the Kassena Nankana Districts of Northern Ghana.
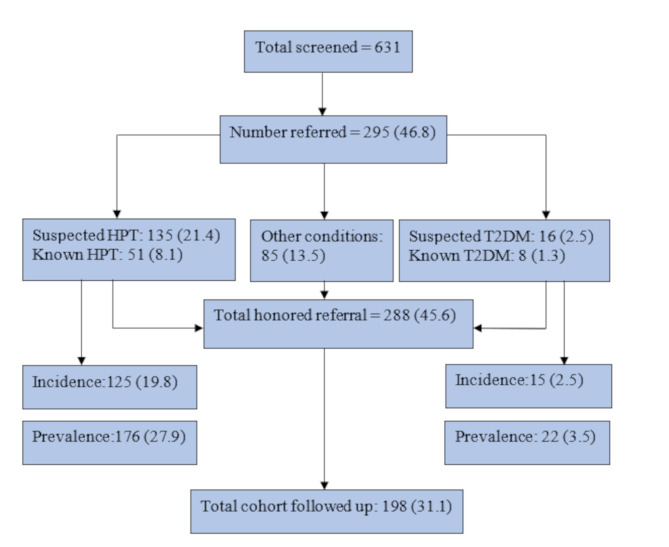
Methods: We screened individuals from 6 FBCs for elevated blood pressure and hyperglycaemia. Suspected hypertension and T2DM cases were referred to health facilities for confirmation and subsequently followed them up for 3 months. We assessed the prevalence of behavioural and metabolic risk factors, including hypertension and T2DM, and the retention of referred cases in the healthcare system over follow up period. We further assessed levels of awareness, treatment and adequate control of hypertension and T2DM.
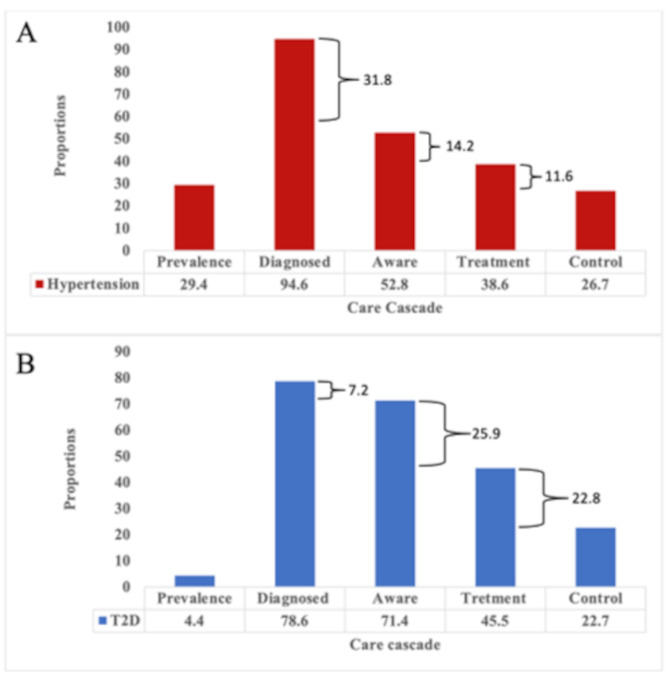
Results: A total of 631 participants were screened, (mean age 49 ± 16years, 73% female) from 6 Faith based Centres. More males than females reported smoking tobacco (14.5% vs. 0.7%) and been physically active (64.5% vs. 52.7%) while more females were obese (29.6 kg/m2 vs. 14.5 kg/m2) and had a higher mean waist circumference (89.0 cm IQR 75-116 cm vs. 84.2 cm IQR 72-107 cm), hip circumference (101.5 ± 10.6 cm vs. 96.4 ± 8.6 cm) and waist-to-hip ratio (0.86 ± 0.1 cm vs. 0.87 ± 0.1 cm) than males. The prevalence of confirmed hypertension and T2DM was 27.9% and 3.5% respectively with no observed sex differences. We observed deficits in the hypertension and T2DM care cascade with reported low awareness, treatment and uncontrolled levels. A 3-month follow up showed a retention in care of 100% in month one and 94.9% in the third month. There was an increase in treatment (39.4% in month-1 and 82.8% in month-3) and control (26.3% in month-1 and 76.3% in month-3) of hypertension and T2DM combined.
Conclusion: Faith-based centres have the potential to enhance the screening, linkage to the healthcare system, and management of hypertension and T2DM. This improvement over the routine system could lead to earlier diagnoses, a reduction in complications, and decreased premature mortality from cardiovascular diseases. Consequently, these efforts would contribute significantly to achieving SDG 3.
Keywords: Diabetes; Faith-based centres; Health Promotion; Hypertension; Primary prevention.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Evaluation of Dyslipidaemia Using an Algorithm of Lipid Profile Measures among Newly Diagnosed Type II Diabetes Mellitus Patients: A Cross-Sectional Study at Dormaa Presbyterian Hospital, Ghana.Medicina (Kaunas). 2019 Jul 21;55(7):392. doi: 10.3390/medicina55070392. Medicina (Kaunas). 2019. PMID: 31330902 Free PMC article.
-
Prevalence of Hypertension and Its Clinical and Psychological Factors in Type 2 Diabetes Patients in Ghana: A Secondary Analysis of a Cross-Sectional Study.J Diabetes Res. 2024 Nov 13;2024:9286774. doi: 10.1155/2024/9286774. eCollection 2024. J Diabetes Res. 2024. PMID: 39568570 Free PMC article.
-
Integration of point-of-care screening for type 2 diabetes mellitus and hypertension into the COVID-19 vaccine programme in Johannesburg, South Africa.BMC Public Health. 2023 Nov 20;23(1):2291. doi: 10.1186/s12889-023-17190-6. BMC Public Health. 2023. PMID: 37986070 Free PMC article.
-
Trends in the Prevalence of Hypertension and Type 2 Diabetes in Bangladesh (2010-2020): A Systematic Review and Meta-Analysis.Curr Diabetes Rev. 2023;19(6):e290422204250. doi: 10.2174/1573399818666220429092805. Curr Diabetes Rev. 2023. PMID: 37183383
-
What is the effect of population-level screening of asymptomatic adults for type 2 diabetes mellitus or intermediate hyperglycaemia on health outcomes? [Internet].Copenhagen: WHO Regional Office for Europe; 2024. Copenhagen: WHO Regional Office for Europe; 2024. PMID: 39133800 Free Books & Documents. Review.
Cited by
-
Implementation of a large-scale hypertension program in primary health centres in the Federal Capital Territory, Nigeria: an explanatory, sequential mixed-methods study.BMJ Open. 2025 Aug 1;15(7):e103121. doi: 10.1136/bmjopen-2025-103121. BMJ Open. 2025. PMID: 40750292 Free PMC article.
References
-
- Kunustor, Powles J. Descriptive epidemiology of blood pressure in a rural adult population in Northern Ghana. Rural Remote Health. 2009;9:1095. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical