

Epidemiology of bronchiectasis at a single center in Japan: a retrospective cohort study
- PMID: 39448945
- PMCID: PMC11520111
- DOI: 10.1186/s12890-024-03337-7
Epidemiology of bronchiectasis at a single center in Japan: a retrospective cohort study
Abstract
Background: The characteristics of bronchiectasis (BE) in Asia, including Japan, remain largely unknown. We aimed to provide insights into the clinical characteristics and treatment outcomes of BE, especially regarding nontuberculous mycobacteria (NTM) infection and its poorly understood impact on prognosis. We also aimed to clarify the effect of long-term macrolide antibiotic use in patients with BE, who had no history of exacerbations.
Methods: In this single-center, retrospective study, the medical records of patients who satisfied the BE criteria between January 1, 2012, and August 31, 2023, were reviewed. Severe exacerbations and mortality during the observation period were recorded. Baseline characteristics and overall survival of patients with and without NTM infection, and factors influencing the time to the first exacerbation and death were analyzed. Additionally, the effects of long-term macrolide antibiotic use in patients without a history of severe exacerbations were estimated.
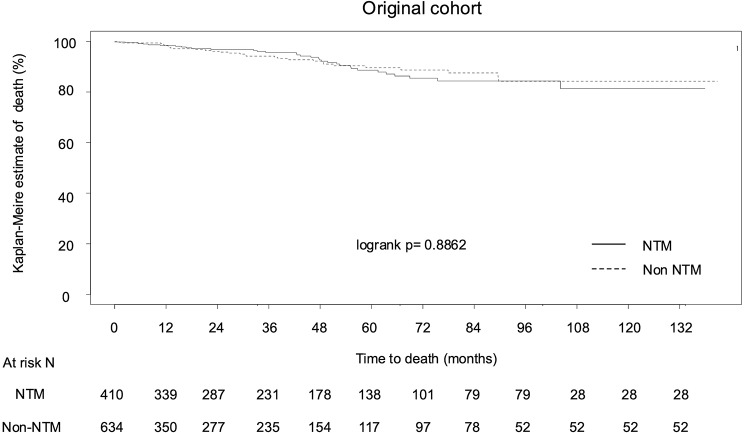
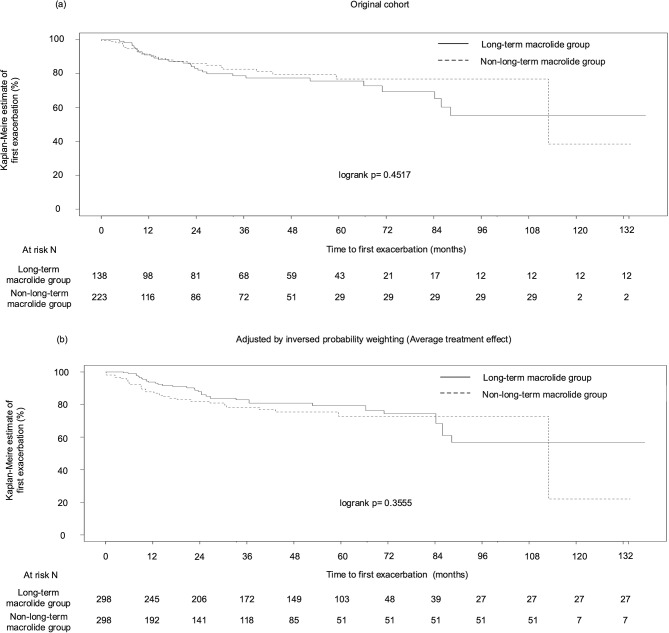
Results: In a cohort of 1044 patients with BE, the rate of severe exacerbation was 22.3%, with mortality rates of 3.2% over 3 years. Notably, the high prevalence of NTM infection (n = 410, 39.3%) in this cohort was distinctive. NTM infection was not associated with either the time to first severe exacerbation (p = 0.5676, adjusted hazard ratio = 1.11) or mortality (p = 0.4139, adjusted hazard ratio = 0.78). Compared with the NTM group, the non-NTM group had a higher proportion of elevated inflammatory markers, with significant differences in C-reactive protein levels (p = 0.0301) and blood neutrophil counts (p = 0.0273). Pseudomonas aeruginosa colonization was more frequent in the non-NTM group (p = 0.0003). Among patients with non-NTM infection and without a history of exacerbation in the past 2 years, 38.2% received long-term macrolide antibiotics that did not invariably prolong the time to first severe exacerbation (p = 0.4517, IPW p = 0.3555).
Conclusions: This study highlights BE epidemiology in Japan, noting that the presence of NTM infection may not necessarily worsen the prognostic outcomes and advising caution in the casual use of macrolides for milder cases without a history of exacerbations.
Clinical trial registration: UMIN Clinical Trials Registry Number: UMIN000054726 (Registered on 21 June 2024).
Keywords: Bronchiectasis; Macrolides; Nontuberculous mycobacteria; TB.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- O’Donnell AE. Bronchiectasis - A clinical review. N Engl J Med. 2022;387:533 – 45. 10.1056/NEJMra2202819, Pubmed:35947710. - PubMed
-
- Kinney WM. Bronchiectasis; a neglected disease. Dis Chest. 1947;13:33–47. 10.1378/chest.13.1.33. Pubmed:20279925. - PubMed
-
- Chalmers JD, Polverino E, Crichton ML, Ringshausen FC, De Soyza A, Vendrell M et al. Bronchiectasis in Europe: data on disease characteristics from the European Bronchiectasis registry (EMBARC). Lancet Respir Med. 2023;11:637 – 49. 10.1016/S2213-2600(23)00093-0, Pubmed:37105206. - PubMed
-
- Kadowaki T, Yano S, Wakabayashi K, Kobayashi K, Ishikawa S, Kimura M, Ikeda T. An analysis of etiology, causal pathogens, imaging patterns, and treatment of Japanese patients with bronchiectasis. Respir Investig. 2015;53:37–44. 10.1016/j.resinv.2014.09.004, Pubmed:25542602. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
