

Spartalizumab in combination with platinum-doublet chemotherapy with or without canakinumab in patients with PD-L1-unselected, metastatic NSCLC
- PMID: 39448966
- PMCID: PMC11515544
- DOI: 10.1186/s12885-024-12841-2
Spartalizumab in combination with platinum-doublet chemotherapy with or without canakinumab in patients with PD-L1-unselected, metastatic NSCLC
Erratum in
-
Correction: Spartalizumab in combination with platinum-doublet chemotherapy with or without canakinumab in patients with PD-L1-unselected, metastatic NSCLC.BMC Cancer. 2024 Nov 21;24(1):1436. doi: 10.1186/s12885-024-13210-9. BMC Cancer. 2024. PMID: 39574037 Free PMC article. No abstract available.
Abstract
Background: Despite promising outcomes of treatment with anti-programmed cell death (PD)-1/PD-ligand (L)1 agents in combination with platinum-doublet chemotherapy (PDC) in the first-line setting, a significant unmet medical need remains in patients with PD-L1-unselected non-small cell lung cancer (NSCLC).
Methods: This multicenter, open-label, phase 1b study comprising dose-confirmation and dose-expansion parts investigated the combination of spartalizumab and various PDC regimens, with or without canakinumab, in treatment-naïve patients with PD-L1-unselected, metastatic NSCLC. The primary objectives were to determine maximum tolerated dose (MTD) and/or recommended dose for expansion (RDE) of spartalizumab, with or without canakinumab, in combination with PDC in the dose-confirmation part and antitumor activity of spartalizumab in the dose-expansion part.
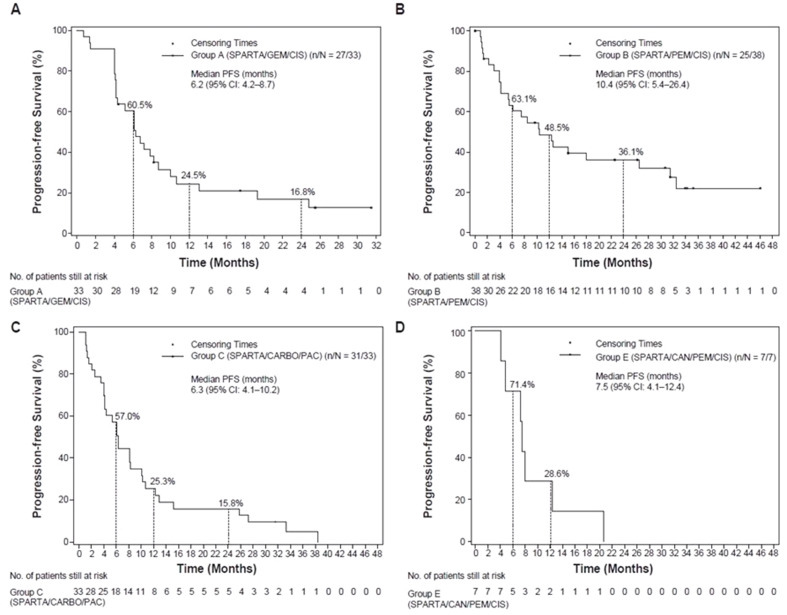
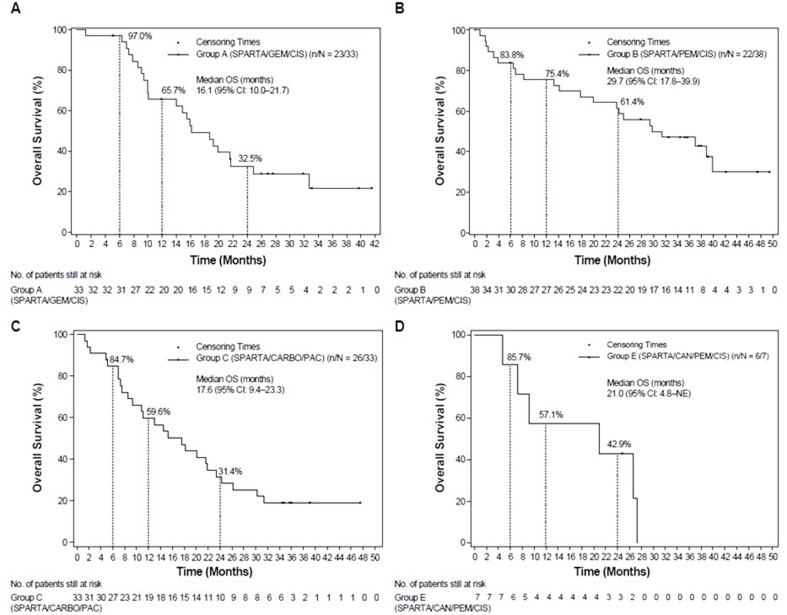
Results: The MTD/RDE of spartalizumab was 300 mg every 3 weeks (Q3W) when administered with either gemcitabine (1250 mg/m2)/cisplatin (75 mg/m2) (group A; no dose-limiting toxicities [DLTs]), pemetrexed (500 mg/m2)/cisplatin (group B; 2 DLTs: grade 2 posterior reversible encephalopathy syndrome and grade 4 hyponatremia), or paclitaxel (200 mg/m2)/carboplatin area under the curve 6 min*mg/mL (group C; 1 DLT: grade 4 neutropenic colitis). The RDE of canakinumab combined with spartalizumab and pemetrexed/cisplatin (group E; no DLTs) was 200 mg Q3W (no dose-expansion part was initiated). No new safety signals were identified. In groups A, B, C, and E, the overall response rates were 57.6%, 55.3%, 51.5%, and 57.1%, respectively. Group B compared with other groups had the longest median progression-free survival (10.4 months vs. 6.2-7.5 months), overall survival (29.7 months vs. 16.1-21.0 months), and duration of response (30.1 months vs. 6.0-8.2 months).
Conclusions: The combination of spartalizumab and PDC, with or without canakinumab, was well tolerated across treatment groups. The antitumor activity across treatment groups was comparable with that of pembrolizumab and pemetrexed combination. Canakinumab did not appear to improve the antitumor activity when combined with spartalizumab, pemetrexed and cisplatin.
Trial registration: The trial was registered in Clinicaltrials.gov with identifier no. NCT03064854. Date of Registration: 06 February 2017.
Keywords: Canakinumab; NSCLC; PD-L1; Platinum-doublet chemotherapy; Spartalizumab.
© 2024. The Author(s).
Conflict of interest statement
AS had been on Advisory Board for BMS, Servier, Gilead, Pfizer, Eisai, BAYER, and MSD, and as consultant for Arqule, Sanofi, Incyte, and served as speaker’s Bureau for Takeda, BMS, Roche, Abbvie, Amgen, Celgene, Servier, Gilead, Astrazeneca, Pfizer, Arqule, Lilly, Sandoz, Eisai, Novartis, BAYER, MSD. GP had served as advisory board member for AbbVie, Amgen, AstraZeneca, Bayer, BMS, GlaxoSmithKline, Janssen, Eli Lilly, MSD, Novartis, Pfizer, Roche, Takeda, Sanofi, Daiichi Sankyo, and Sanofi. He has received financial support and speaker fees from AstraZeneca, Janssen, MSD, Novartis, Pfizer, Roche, Takeda, Blue Print, Apollomics, Amgen, Array Biopharma, IO Biotech. GP received other personal financial interests from Lung Cancer Medical Education TASC Committee from Janssen. In terms of non-financial interests, GP has held leadership roles as a council member for the Women for Oncology Committee Chair Fellowship and Award Committee, and Press Committee Faculty for lung and other thoracic tumors for ESMO. He has served as the President of the Spanish Federation of Medical Societies (FACME) from 2020 – 2022 and currently from 2023 – 2024. He is the former President of the Spanish Medical Oncology Society (SEOM), and a member and board member of the Scientific Committee of the Spanish Against Cancer Research Foundation (AECC), member of the IASLC Women in Thoracic Oncology Working Group. GP has advisory roles as a member of the Spanish National Health Advisory Board for the Spanish Minister of Health, advisory role for lung cancer screening evaluation for EUnetHTA, Spanish National Evaluation network (RedETS), and for EMA. DSWT received honoraria from Amgen, Bayer, Merck, Pfizer, Novartis, Boehringer, Ingelheim, Roche, Takeda. He has served as a consultant and advisory role for Amgen, Astra Zeneca, Bayer, Boehringer Ingelheim, DKSH, GlaxoSmithKline, Merck, Novartis, Pfizer, Roche and Takeda. He has received research grants from ACM Biolabs, Amgen, Astra Zeneca, Bayer and Pfizer outside this work. JZ reports personal fees from Sanofi, MSD, NanoString, Pfizer, and Novartis outside the submitted work; grants and personal fees from BMS, AstraZeneca, and Roche. AB has served as a consultant or on advisory boards for Amgen, AstraZeneca, Bristol Myers Squibb (BMS), Janssen, Merck, Novartis, Pfizer, Roche/Genentech, Sanofi, and Takeda. AB received fees for speaking and travels from Pfizer, Takeda, Roche, MERCK SHARP & DOHME (MSD). FB has no personal financial interests (since August 2021); Institutional financial interests from Abbvie, ACEA, Amgen, Astrazeneca, Bayer, BMS, Boehringer–Ingelheim, Eisai, Eli Lilly Oncology, F. Hoffmann–La Roche Ltd, Genentech, Ipsen, Ignyta, Innate Pharma, Loxo, Novartis, Medimmune, Merck, MSD, Pierre Fabre, Pfizer, Sanofi-Aventis and Takeda; Non-financial interests as Principal Investigator for Astra-Zeneca, BMS, Innate Pharma, Merck, Pierre Fabre and F. Hoffmann-La Roche, Ltd, sponsored trials (or ISR).TMK received consulting fees or honoraria for lectures from AstraZeneca, IMBDx, Inc., Janssen, Regeneron, Samsung Bioepis, Takeda, and Yuhan; had advisory role at AstraZeneca, Janssen, Regeneron, and Takeda; and received research grant from AstraZeneca-KHIDI outside this work. TRO received grants as an advisor or speaker from: AstraZeneca, Boehringer Ingelheim, Daiichi-Sankyo, Roche Pharma, Merck Sharp and Dohme, Novartis Pharma and Takeda Oncology, TRO received travel support from AstraZeneca and Janssen-Cilag.EF served on advisory boards for Abbvie, Amgen, Astra Zeneca, Bayer, Beigene, Boehringer Ingelheim, Bristol Myers Squibb, Eli Lilly, F. Hoffmann-La Roche, Gilead, Glaxo Smith Kline, Janssen, Merck Serono, Merck Sharp & Dohme, Novartis, Peptomyc, Pfizer, Regeneron, Sanofim Takeda, Turning Point, Daiichi Sankyo. EF has received speaker fees from Amgen, Astra Zeneca, Bristol Myers Squibb, Daiichi Sankyo, Eli Lilly, F. Hoffmann- La Roche, Genentech, Janssen, Medical Trensa, Medscape, Merck Serono, Merck Sharp & Dohme, Peervoice, Pfizer, Sanofi, Takeda, and Touch Oncology. EF was a board member of Grifols. FAS and ESS do not have any competing interests to disclose. CC, ES, TM are employees of Novartis. TM holds shares with Novartis.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA: A Cancer Journal for Clinicians 2021;71(1):7–33. - PubMed
-
- Barlesi F, Scherpereel A, Rittmeyer A, Pazzola A, Ferrer Tur N, Kim JH, et al. Randomized phase III trial of maintenance bevacizumab with or without pemetrexed after first-line induction with bevacizumab, cisplatin, and pemetrexed in advanced nonsquamous non-small-cell lung cancer: AVAPERL (MO22089). J Clin Oncol. 2013;31(24):3004–11. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
