

Aromatase, testosterone, TMPRSS2: determinants of COVID-19 severity
- PMID: 39449074
- PMCID: PMC11515603
- DOI: 10.1186/s13293-024-00658-4
Aromatase, testosterone, TMPRSS2: determinants of COVID-19 severity
Abstract
Background: Male sex has been identified as a risk factor for worse COVID-19 outcomes. This sex difference has been mostly attributed to the complex role of sex hormones. Cell surface entry of SARS-CoV-2 is mediated by the transmembrane protease serine 2 (TMPRSS2) which is under transcriptional regulation by androgens. P450 aromatase enzyme converts androgens to estrogens. This study measured concentrations of aromatase enzyme, testosterone, estradiol, and TMPRSS-2 in plasma of hospitalized COVID-19 patients to elucidate the dynamics of sex-linked disparity in COVID-19 and correlate them with disease severity and mortality.
Methods: In this prospective cohort study, a total of 265 patients (41% women), age 18 years and older, who had a positive COVID-19 PCR test and were hospitalized for COVID-19 at Memorial Hermann Hospital in Houston, (between May 2020 and May 2021) were enrolled in the study if met inclusion criteria. Plasma concentrations of Testosterone, aromatase, TMPRSS-2, and estradiol were measured by ELISA. COVID-19 patients were dichotomized based on disease severity into moderate-severe (n = 146) or critical (n = 119). Mann Whitney U and logistic regression were used to correlate the analytes with disease severity and mortality.
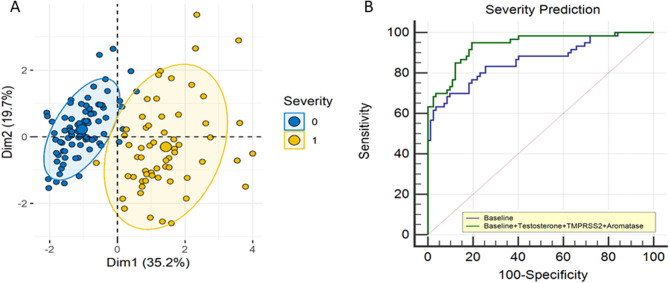
Results: TMPRSS2 (2.5 ± 0.31 vs. 1.73 ± 0.21 ng/mL, p < 0.01) and testosterone (1.2 ± 0.1 vs. 0.44 ± 0.12 ng/mL, p < 0.01) were significantly higher in men as compared to women with COVID-19 after adjusting for age in a multivariate model. There was no sex difference seen in the level of estradiol and aromatase in COVID-19 patients. TMPRSS2 and aromatase were higher, while testosterone was lower in patients with increased COVID-19 severity. They were independently associated with COVID-19 severity, after adjusting for several baseline risk factors in a multivariate logistic regression model. In terms of mortality, TMPRRS2 and aromatase levels were significantly higher in non-survivors.
Conclusions: Our study demonstrates that testosterone, aromatase, and TMPRSS2 are markers of COVID-19 severity. Estradiol levels do not change with disease severity in COVID-19. In terms of mortality prediction, higher aromatase and TMPRSS-2 levels can be used to predict mortality from COVID-19 in hospitalized patients. COVID-19 has caused over a million deaths in the U.S., with men often getting sicker than women. Testosterone, a male hormone, helps control a protein called TMPRSS-2, which allows the COVID-19 virus to spread more easily in the body. A protein called aromatase converts the male hormone testosterone into the female hormone estrogen. It is thought that female hormone estrogen helps protect women from getting seriously ill from COVID-19. To understand the role of these hormones in COVID-19 and sex differences, we measured levels of testosterone, estrogen, aromatase (which turns testosterone into estrogen), and TMPRSS-2 in hospitalized COVID-19 patients. We also checked how this level might reflect the severity of the disease. We found that critically ill COVID-19 patients (the ones in ICU) had higher levels of TMPRSS-2 and aromatase, and lower testosterone levels. When we used these hormone levels to predict death in hospitalized COVID-19 patients, higher levels of TMPRSS-2 and aromatase were linked to a lower chance of survival.
Keywords: Aromatase; COVID-19; CRP; Sex differences.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Clinical Management. of COVID-19: Living GuidelineWorld Health Organization, Geneva,. (2022). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
