

Comments and Illustrations of the European Federation of Societies for Ultrasound in Medicine (EFSUMB) Guidelines: Rare Malignant Pulmonal and Pleural Tumors: Primary Pulmonary Sarcoma and Mesothelioma, Imaging Features on Transthoracic Ultrasound
- PMID: 39451662
- PMCID: PMC11506974
- DOI: 10.3390/diagnostics14202339
Comments and Illustrations of the European Federation of Societies for Ultrasound in Medicine (EFSUMB) Guidelines: Rare Malignant Pulmonal and Pleural Tumors: Primary Pulmonary Sarcoma and Mesothelioma, Imaging Features on Transthoracic Ultrasound
Abstract
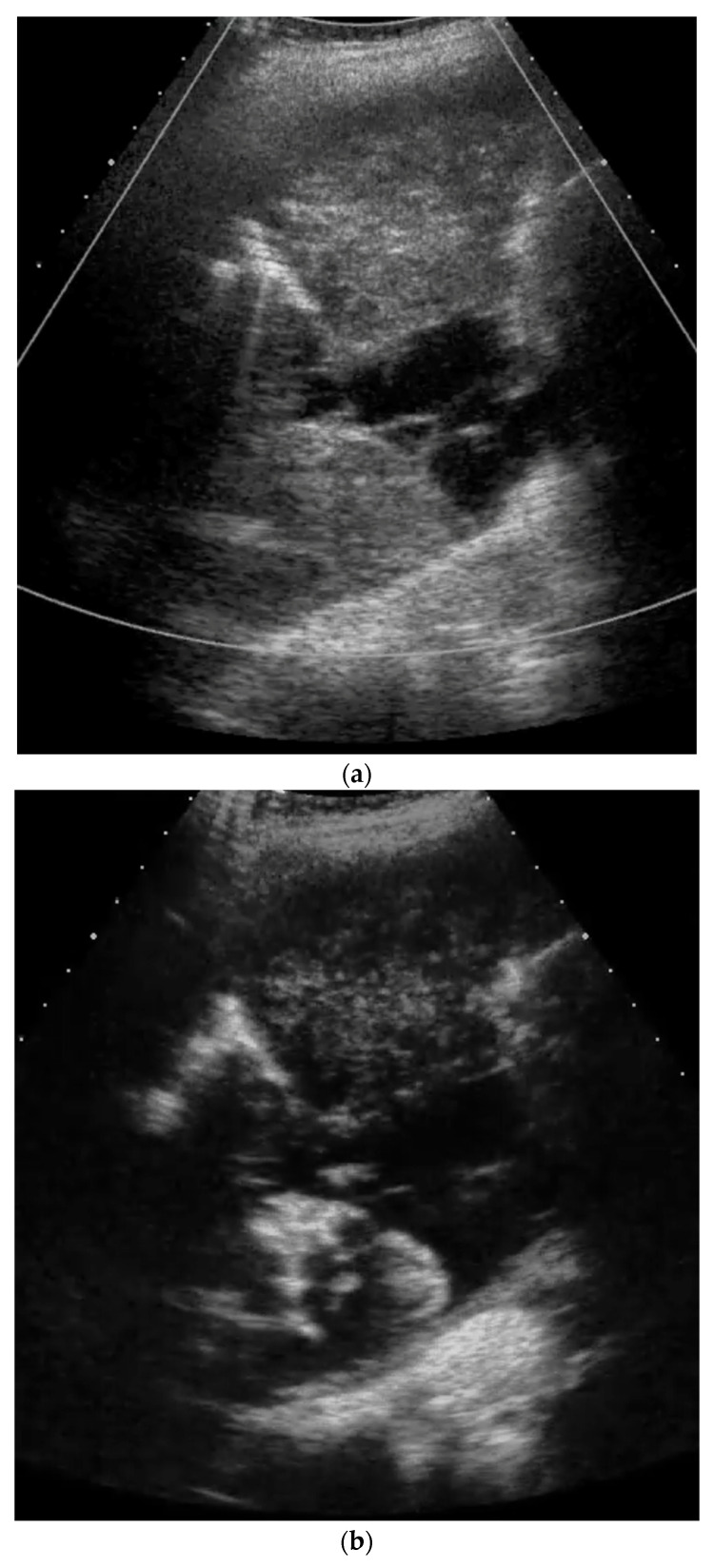
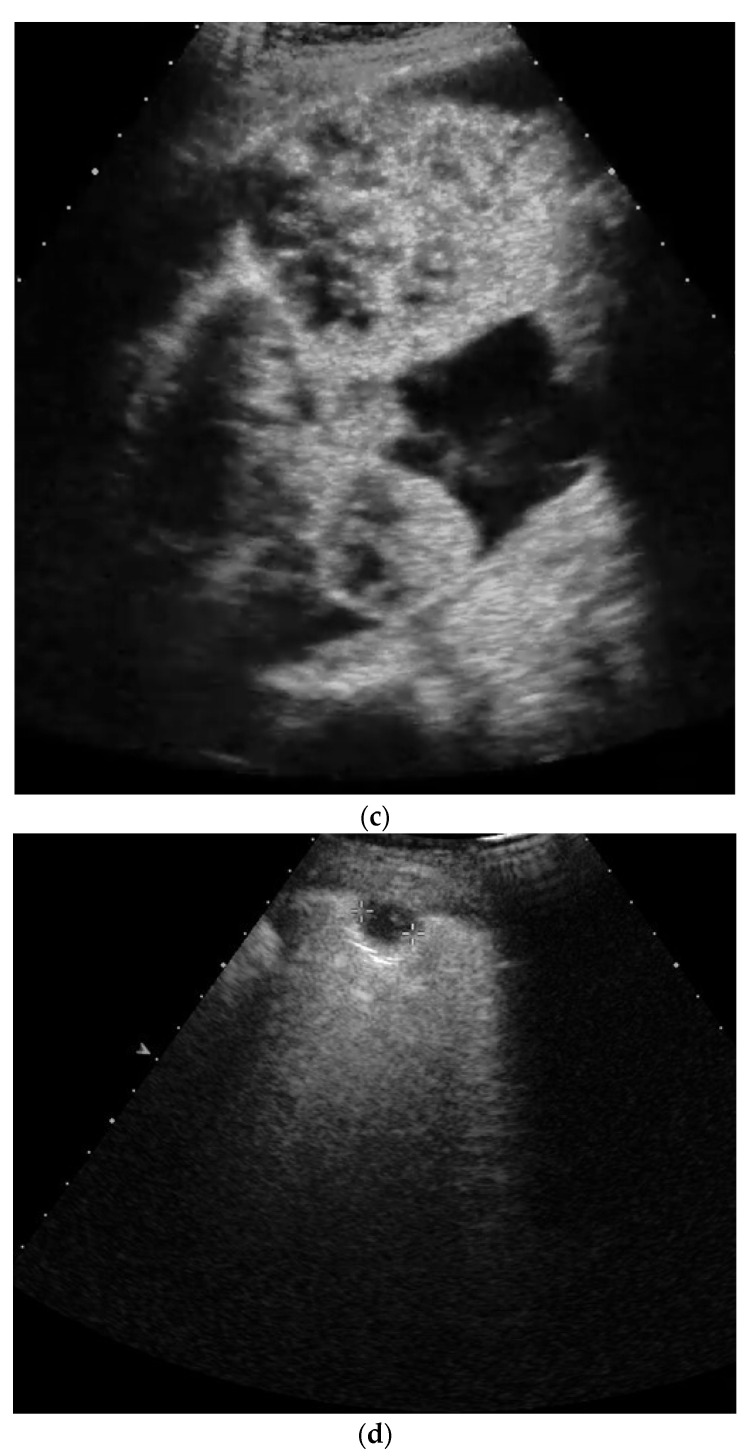
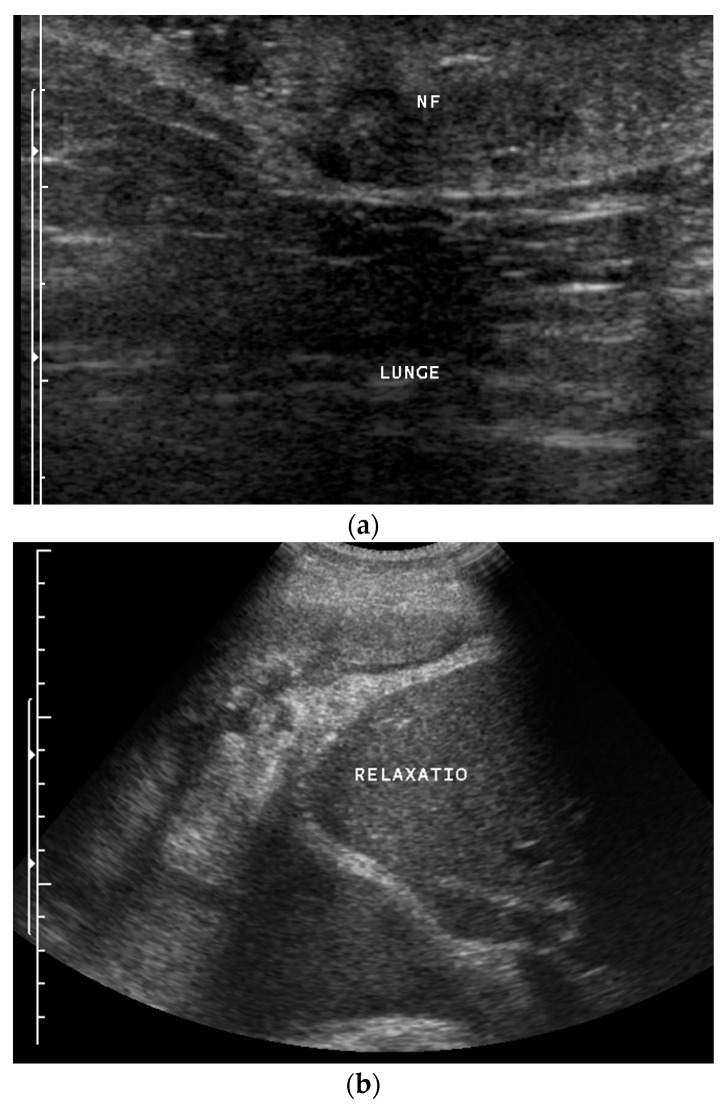
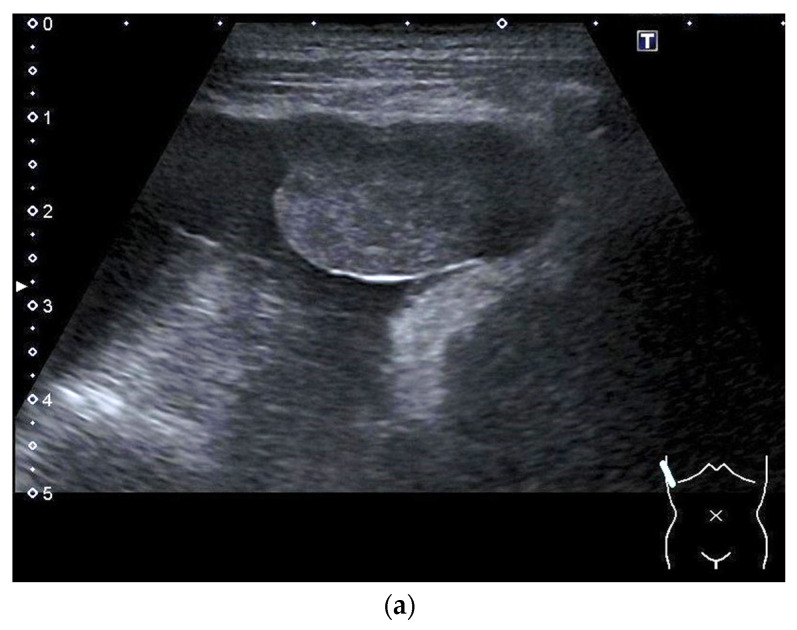
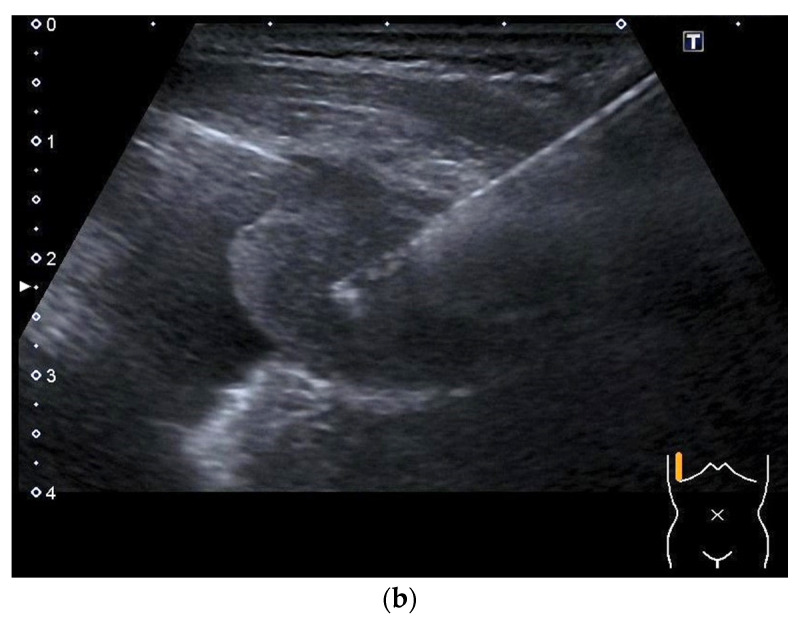
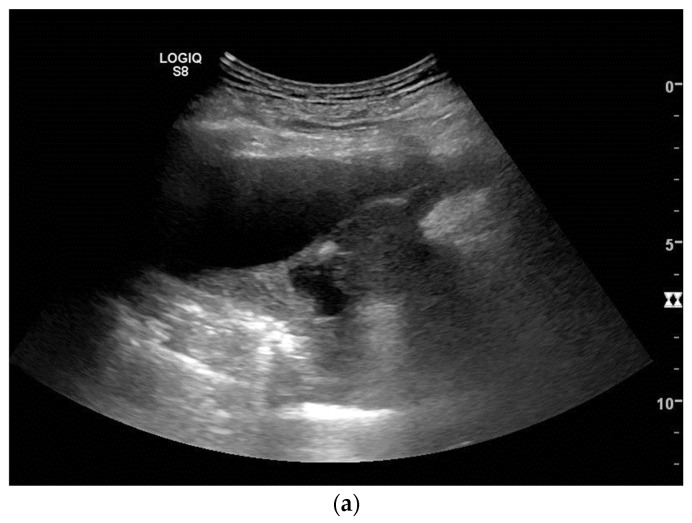
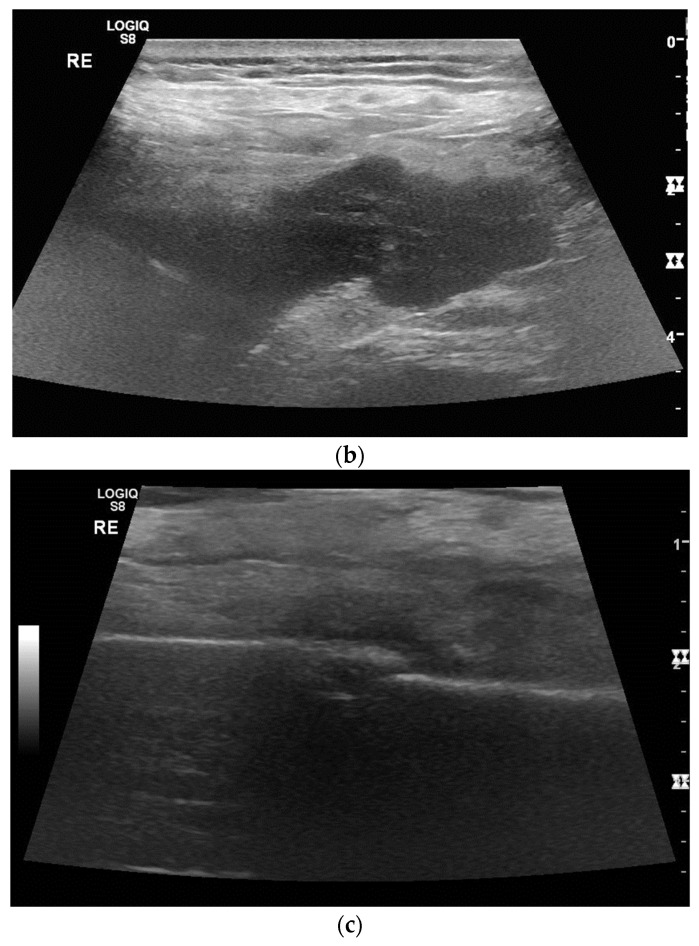
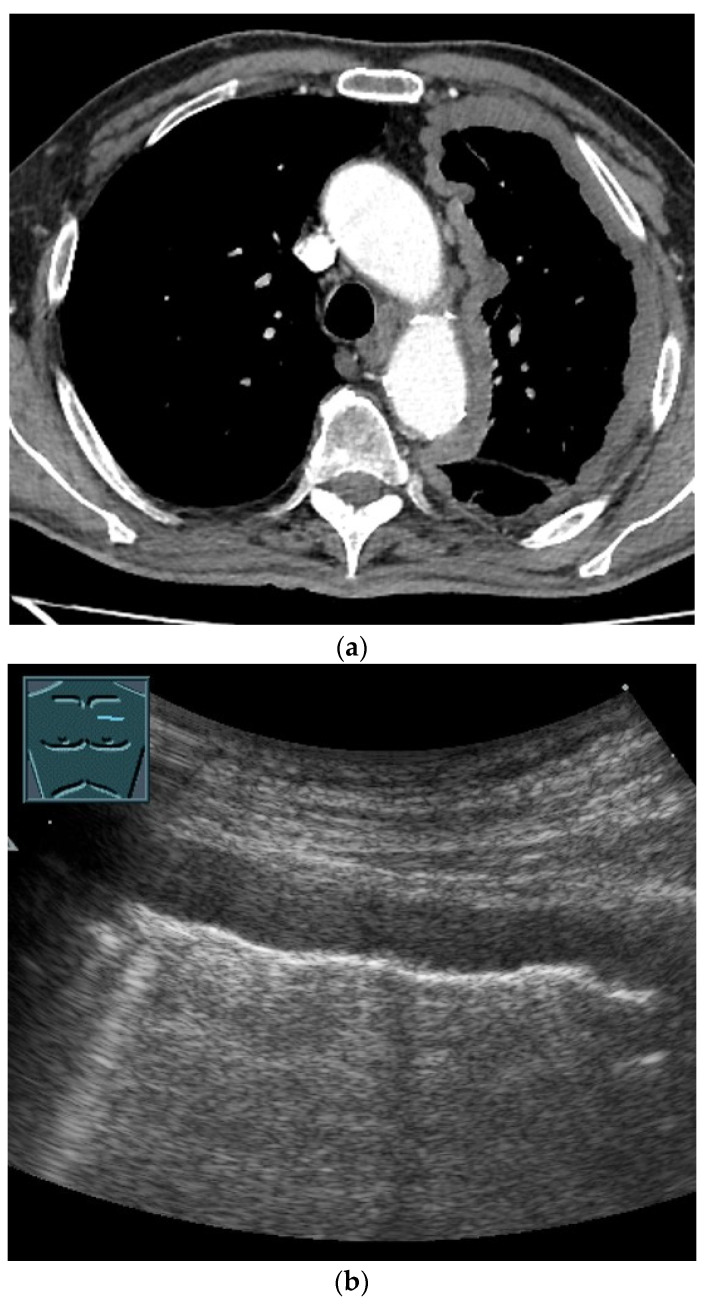
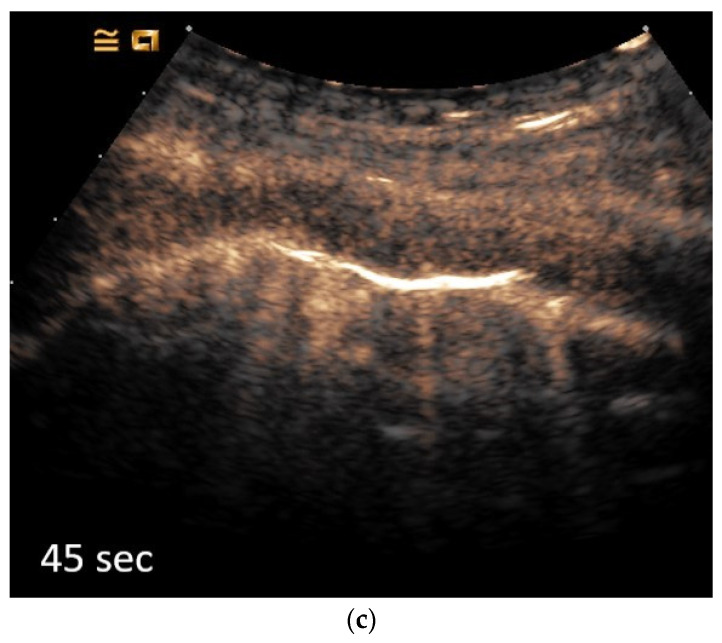
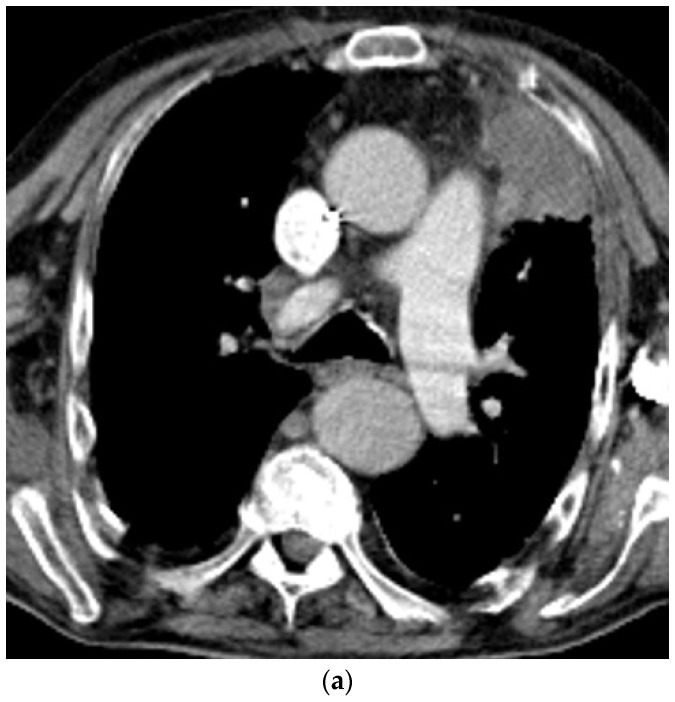
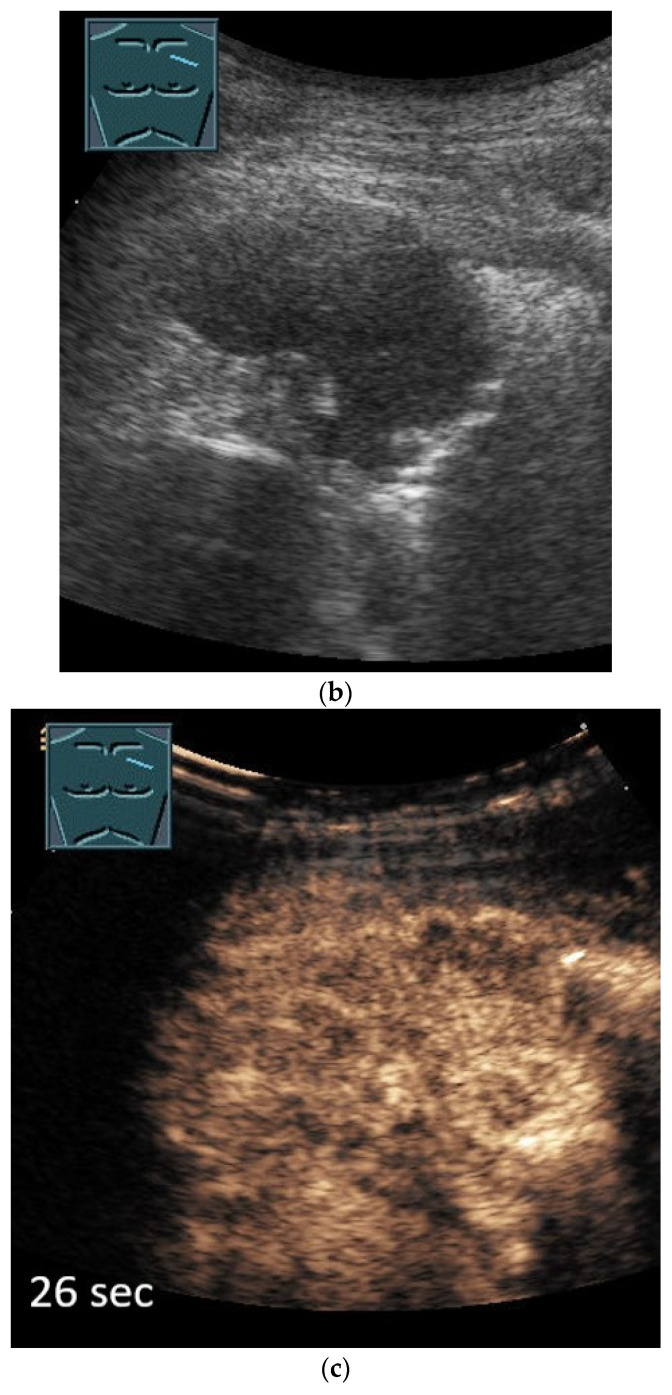
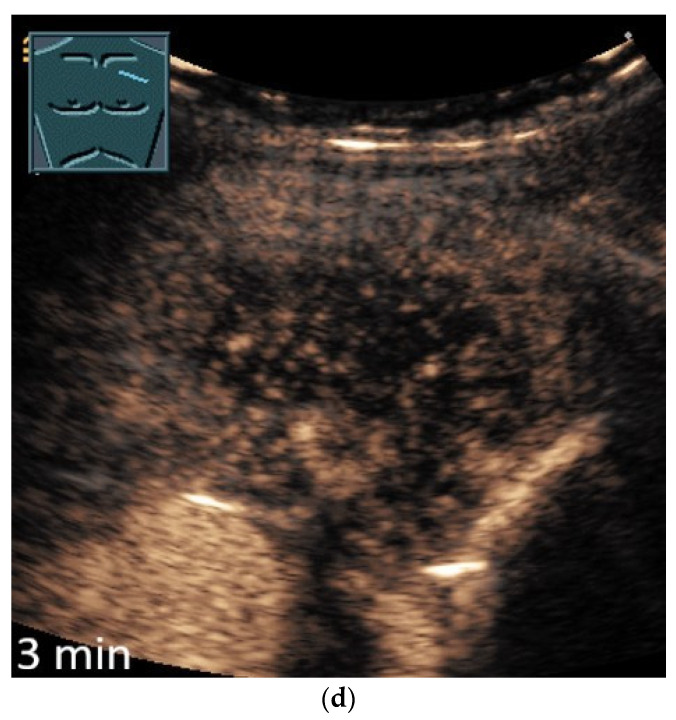
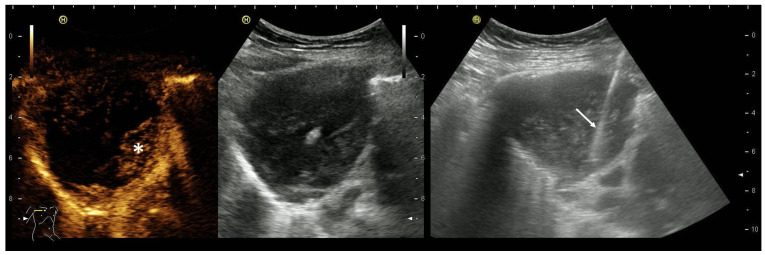
Primary pulmonary sarcoma and mesothelioma are rare malignancies. The review article discusses the appearance of these tumors in B-mode ultrasound (US), color Doppler ultrasound and contrast-enhanced ultrasound (CEUS). In particular, the article is intended to inspire the examination of thoracic wall tumors and pleural masses with the possibilities of ultrasonography and to obtain histologically evaluable material using US or CEUS-guided sampling.
Keywords: advances; contrast-enhanced ultrasound; diagnosis; imaging; lung ultrasound; respiratory medicine.
Conflict of interest statement
The authors declare that they have no financial conflict of interest with regard to the content of this report. Some authors have received financial support and/or honoraria from Bracco for the organization of ultrasound courses. In addition, some authors have been supported with equipment from various ultrasound equipment companies for the organization of ultrasound courses and/or have received honoraria for lectures.
Figures
Similar articles
-
Comments and Illustrations of the European Federation of Societies for Ultrasound in Medicine Guidelines: Benign Pleura Lesions (Benign Pleura Thickening, Lesions and Masses)-What Can Be Seen on Transthoracic Ultrasound?Diagnostics (Basel). 2025 Jan 14;15(2):176. doi: 10.3390/diagnostics15020176. Diagnostics (Basel). 2025. PMID: 39857060 Free PMC article. Review.
-
Comments and illustrations of the European Federation of Societies for Ultrasound in Medicine contrast-enhanced ultrasonography guidelines: multiparametric imaging and EUS-guided sampling in rare pancreatic tumors. Mesenchymal pancreatic tumors of intermediate biological behaviour.Endosc Ultrasound. 2024 May-Jun;13(3):145-153. doi: 10.1097/eus.0000000000000071. Epub 2024 Jul 5. Endosc Ultrasound. 2024. PMID: 39318650 Free PMC article.
-
Comments and illustrations of the European Federation of Societies for Ultrasound in Medicine contrast-enhanced ultrasound guidelines: Multiparametric imaging and EUS-guided sampling in rare pancreatic tumors. Benign mesenchymal pancreatic tumors.Endosc Ultrasound. 2024 Jul-Aug;13(4):218-231. doi: 10.1097/eus.0000000000000070. Epub 2024 Aug 16. Endosc Ultrasound. 2024. PMID: 39318747 Free PMC article.
-
History of Ultrasound in Medicine from its birth to date (2022), on occasion of the 50 Years Anniversary of EFSUMB. A publication of the European Federation of Societies for Ultrasound In Medicine and Biology (EFSUMB), designed to record the historical development of medical ultrasound.Med Ultrason. 2022 Dec 21;24(4):434-450. doi: 10.11152/mu-3757. Epub 2022 May 15. Med Ultrason. 2022. PMID: 35574917 Review.
-
Comments on and Illustrations of the EFSUMB CEUS Guidelines: Transabdominal and Endoscopic Ultrasound Features of Intrapancreatic Metastases and the Role of Multiparametric Imaging and EUS-Guided Sampling in Rare Pancreatic Tumors.Cancers (Basel). 2023 Apr 29;15(9):2546. doi: 10.3390/cancers15092546. Cancers (Basel). 2023. PMID: 37174015 Free PMC article. Review.
Cited by
-
Mesothelioma of the Tunica Vaginalis Testis: Diagnostic and Therapeutic Management. A Comprehensive Review, 1982-2024.Cancers (Basel). 2024 Nov 26;16(23):3956. doi: 10.3390/cancers16233956. Cancers (Basel). 2024. PMID: 39682143 Free PMC article. Review.
-
Comments and Illustrations of the European Federation of Societies for Ultrasound in Medicine Guidelines: Benign Pleura Lesions (Benign Pleura Thickening, Lesions and Masses)-What Can Be Seen on Transthoracic Ultrasound?Diagnostics (Basel). 2025 Jan 14;15(2):176. doi: 10.3390/diagnostics15020176. Diagnostics (Basel). 2025. PMID: 39857060 Free PMC article. Review.
References
-
- Safai Zadeh E., Gorg C., Prosch H., Horn R., Jenssen C., Dietrich C.F. The Role of Thoracic Ultrasound for Diagnosis of Diseases of the Chest Wall, the Mediastinum, and the Diaphragm-Narrative Review and Pictorial Essay. Diagnostics. 2023;13:767. doi: 10.3390/diagnostics13040767. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
