

Aesthetical and Functional Rehabilitation for an Ankylosed Maxillary Canine-A Case Report
- PMID: 39451874
- PMCID: PMC11506519
- DOI: 10.3390/clinpract14050159
Aesthetical and Functional Rehabilitation for an Ankylosed Maxillary Canine-A Case Report
Abstract
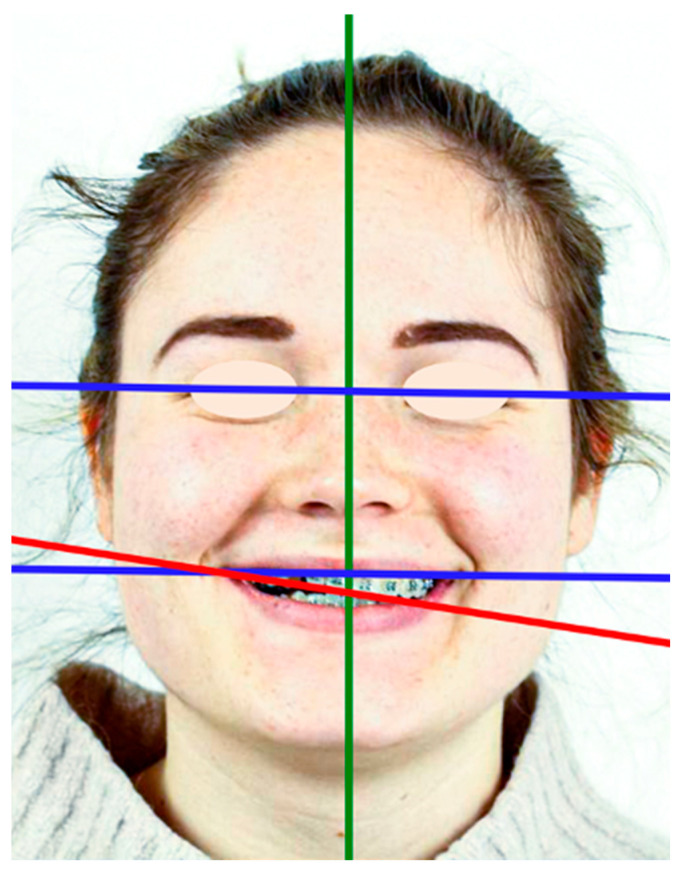
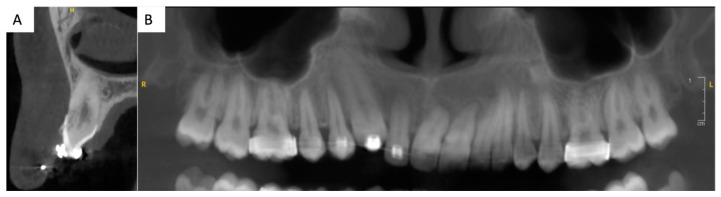
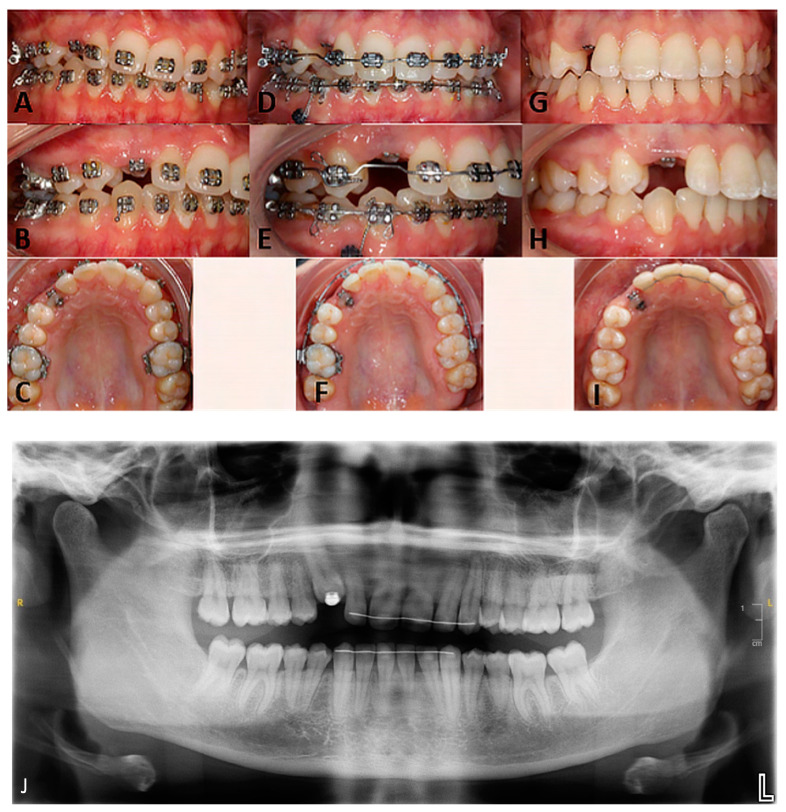
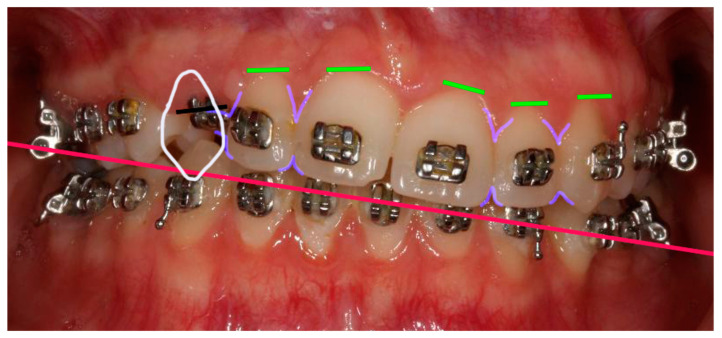
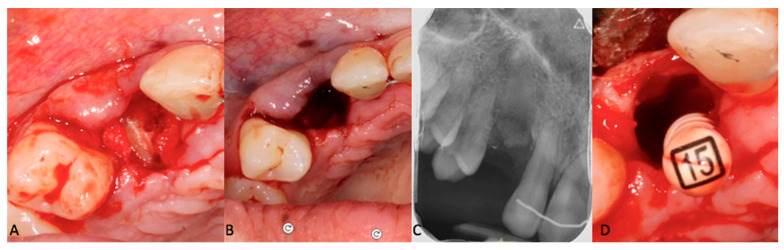
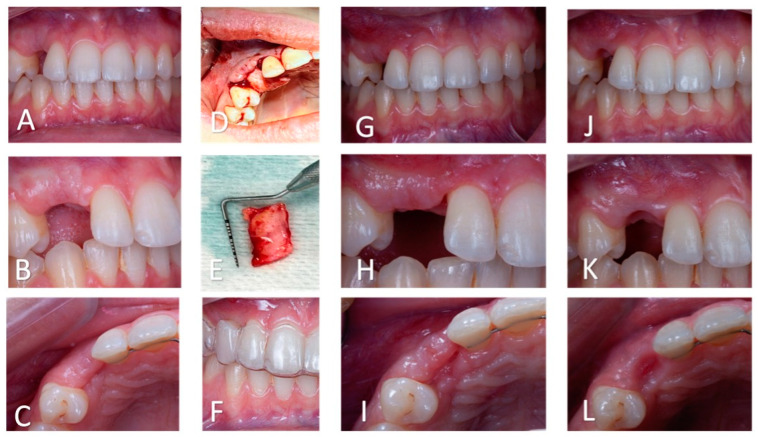
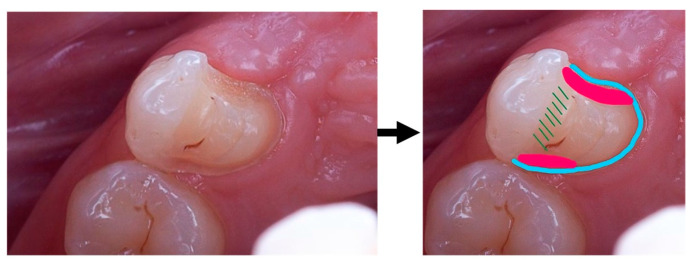
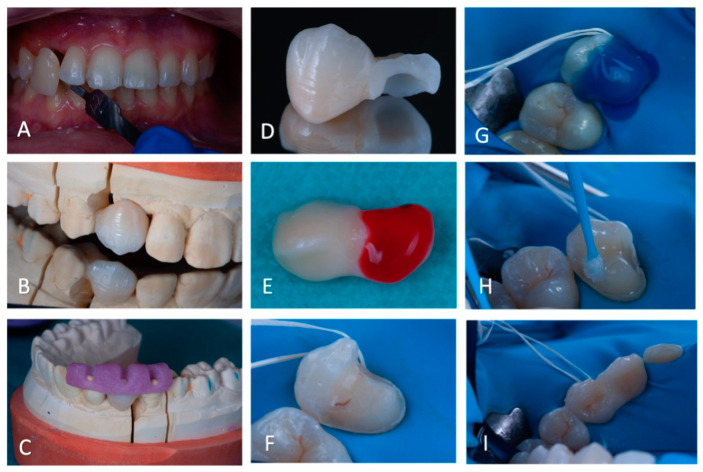
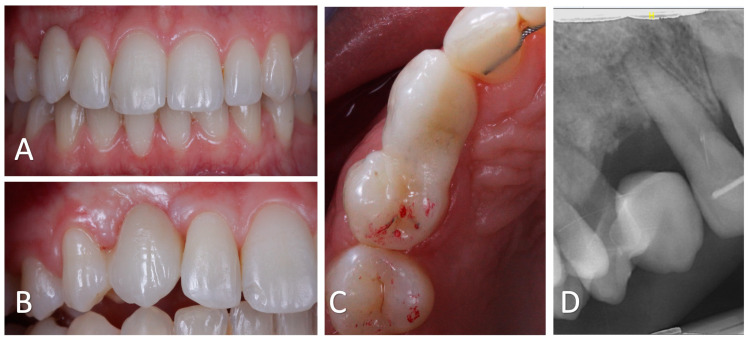
Background: As the functional and aesthetical importance of the canine cannot be overstated, the management of a missing canine is challenging. This case report describes the treatment of an infra-occluded ankylosed maxillary canine in a patient with previously failed orthodontic treatment. Case description: A 20-year-old patient sought a second opinion for orthodontic treatment failure. The patient presented with an impacted, ankylosed, and severely infra-occluded right maxillary canine, as well as an iatrogenic clockwise cant of the maxillary occlusal plane and several root resorptions. The treatment corrected the cant of the occlusal plane while avoiding further root resorption, partially extracted the upper right canine, improved the quality and quantity of the soft tissue in the newly edentulous area, and provided a prosthetic rehabilitation using a lithium disilicate ceramic resin-bonded cantilever bridge. Conclusions: The use of a cantilevered bridge resulted in an aesthetically pleasing and minimally invasive rehabilitation. This technique is reversible, does not affect pulp vitality, and is a viable solution for rehabilitating the smiles of young patients. Clinical significance: The smile rehabilitation for an ankylosed maxillary canine, especially in the case of a previously failed orthodontic treatment, is an important clinical challenge. A minimally invasive long-term restoration with a cantilever bridge is a viable solution. Functional and aesthetically pleasant results can be achieved with a multidisciplinary approach.
Keywords: ankylosed tooth; canine ankylosis; cantilever bridge; case report; decoronation; occlusal plane cant; root resorption.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


References
-
- Parrish J., Hills L., Ganesan K. Management of palatally ectopic canines part 2: Ankylosis hypotheses and southend experience. Adv. Mech. Mach. Sci. 2022;8:100349. doi: 10.1016/j.adoms.2022.100349. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
