

Nanofat Improves Vascularization and Tissue Integration of Dermal Substitutes without Affecting Their Biocompatibility
- PMID: 39452592
- PMCID: PMC11508499
- DOI: 10.3390/jfb15100294
Nanofat Improves Vascularization and Tissue Integration of Dermal Substitutes without Affecting Their Biocompatibility
Abstract
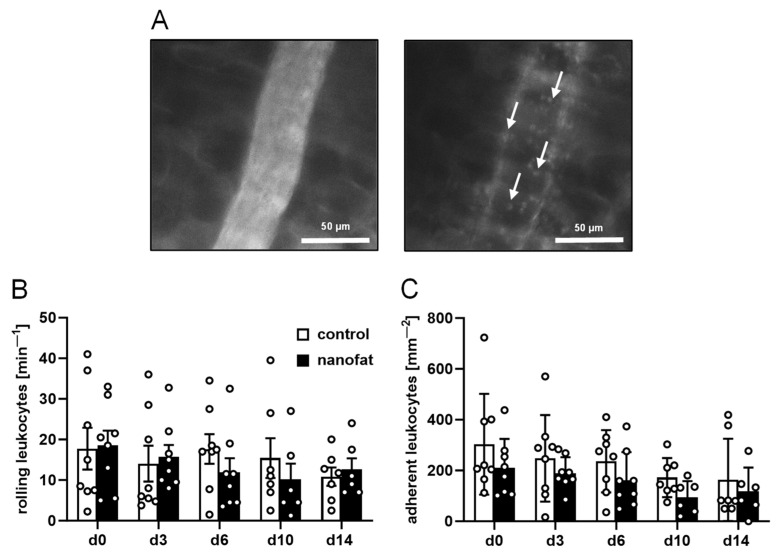
Dermal substitutes require sufficient tissue integration and vascularization to be successfully covered with split-thickness skin grafts. To rapidly achieve this, we provide the proof of principle for a novel vascularization strategy with high translational potential. Nanofat was generated from subcutaneous adipose tissue of green fluorescence protein (GFP)+ C57BL/6J donor mice and seeded onto small samples (4 mm in diameter) of the clinically approved dermal substitute Integra®. These samples and non-seeded controls were then implanted into full-thickness skin defects in the dorsal skinfold chamber of C57BL/6J wild-type mice and analyzed by intravital fluorescence microscopy, histology and immunohistochemistry over a 14-day period. Nanofat-seeded dermal substitutes exhibited an accelerated vascularization, as indicated by a significantly higher functional microvessel density on days 10 and 14 when compared to controls. This was primarily caused by the reassembly of GFP+ microvascular fragments inside the nanofat into microvascular networks. The improved vascularization promoted integration of the implants into the surrounding host tissue, which finally exhibited an increased formation of a collagen-rich granulation tissue. There were no marked differences in the inflammatory host tissue reaction to nanofat-seeded and control implants. These findings demonstrate that nanofat significantly improves the in vivo performance of dermal substitutes without affecting their biocompatibility.
Keywords: Integra®; angiogenesis; dermal substitutes; inflammation; nanofat; skin regeneration; vascularization.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures






References
LinkOut - more resources
Full Text Sources
